COVID-19 Situation Update
Monday 31st January 2022
| Transmission Update:
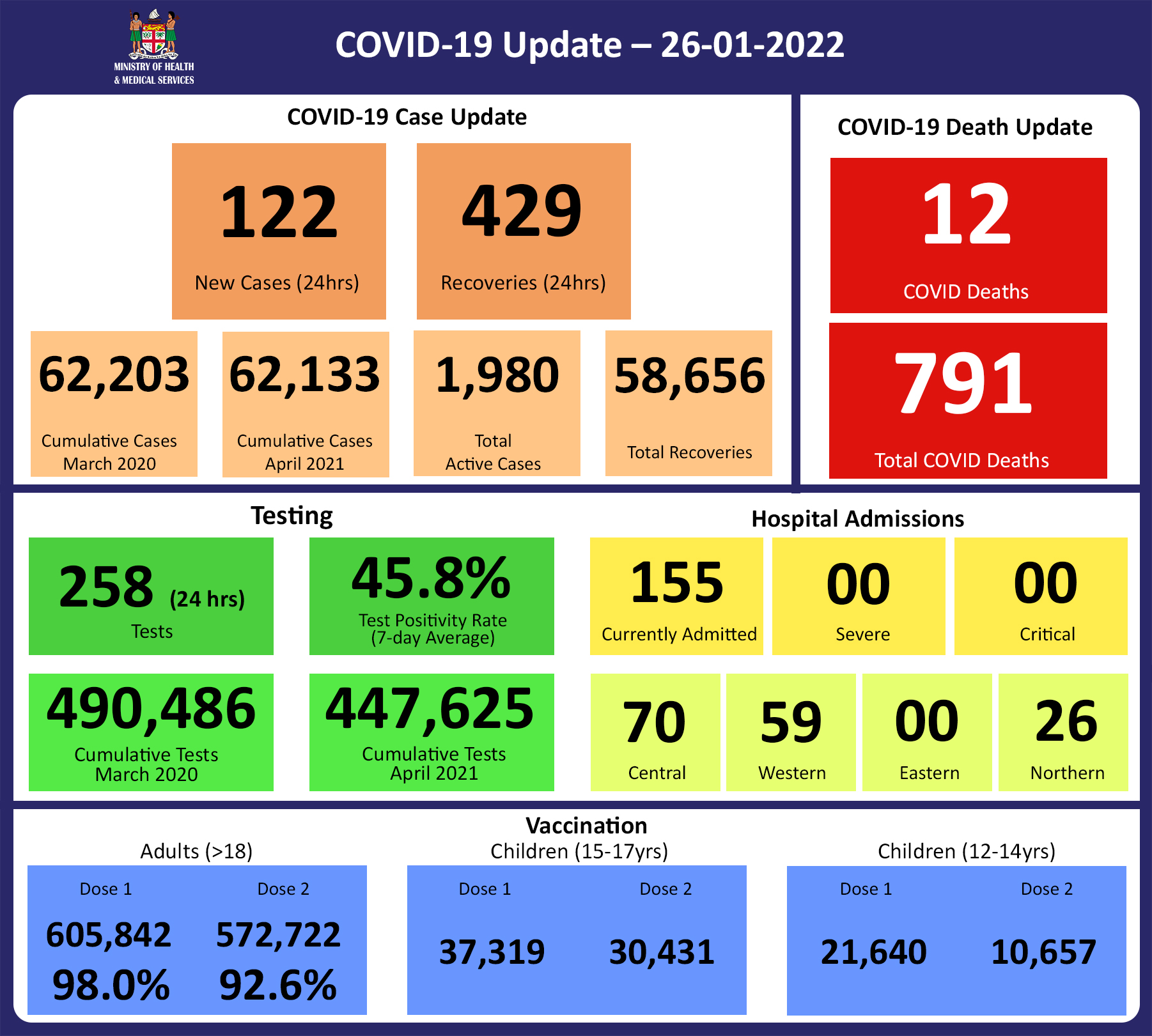
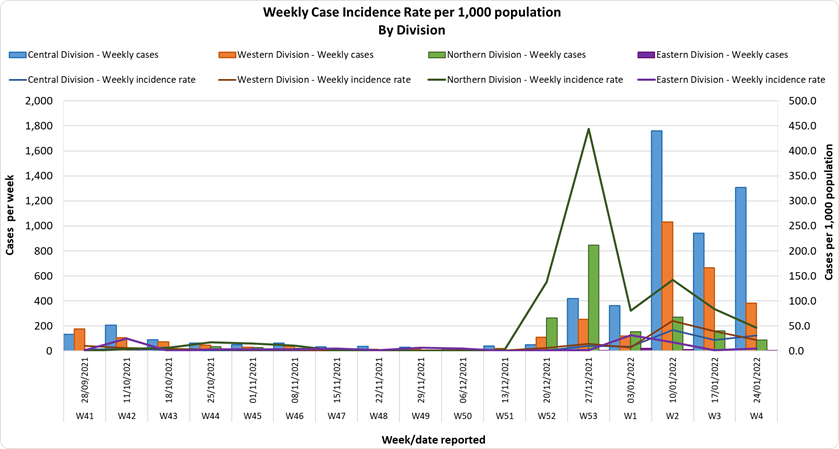
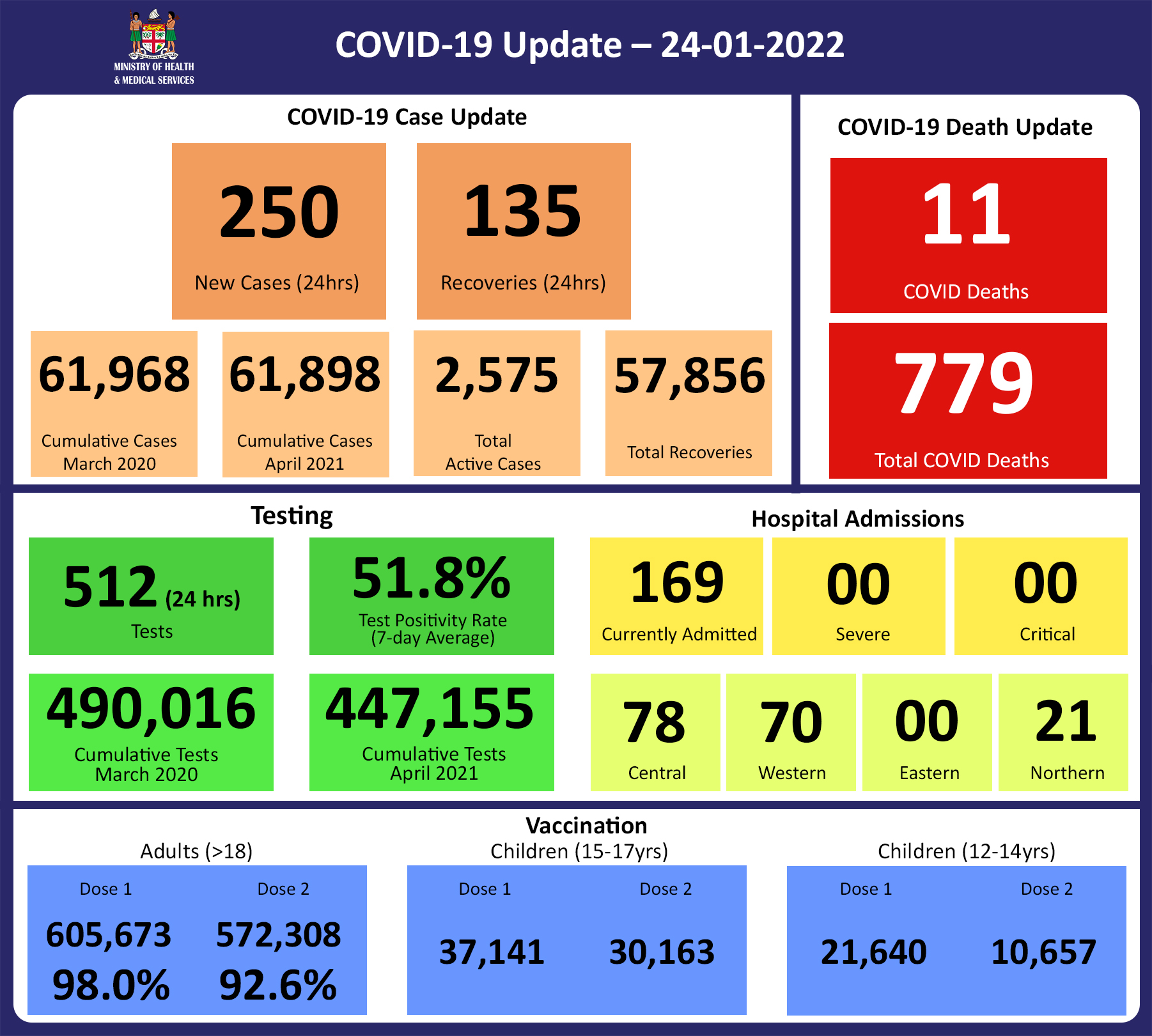
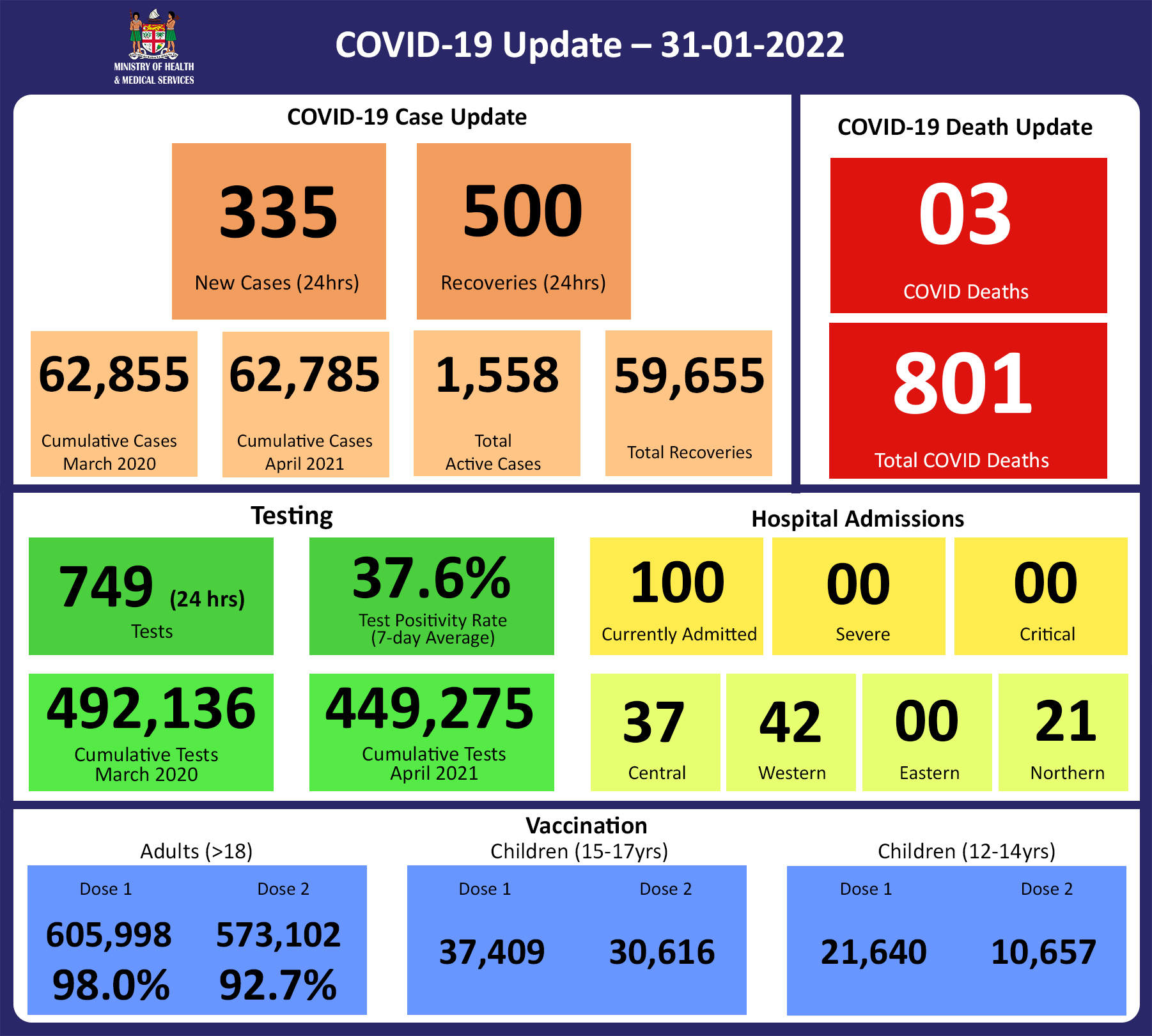
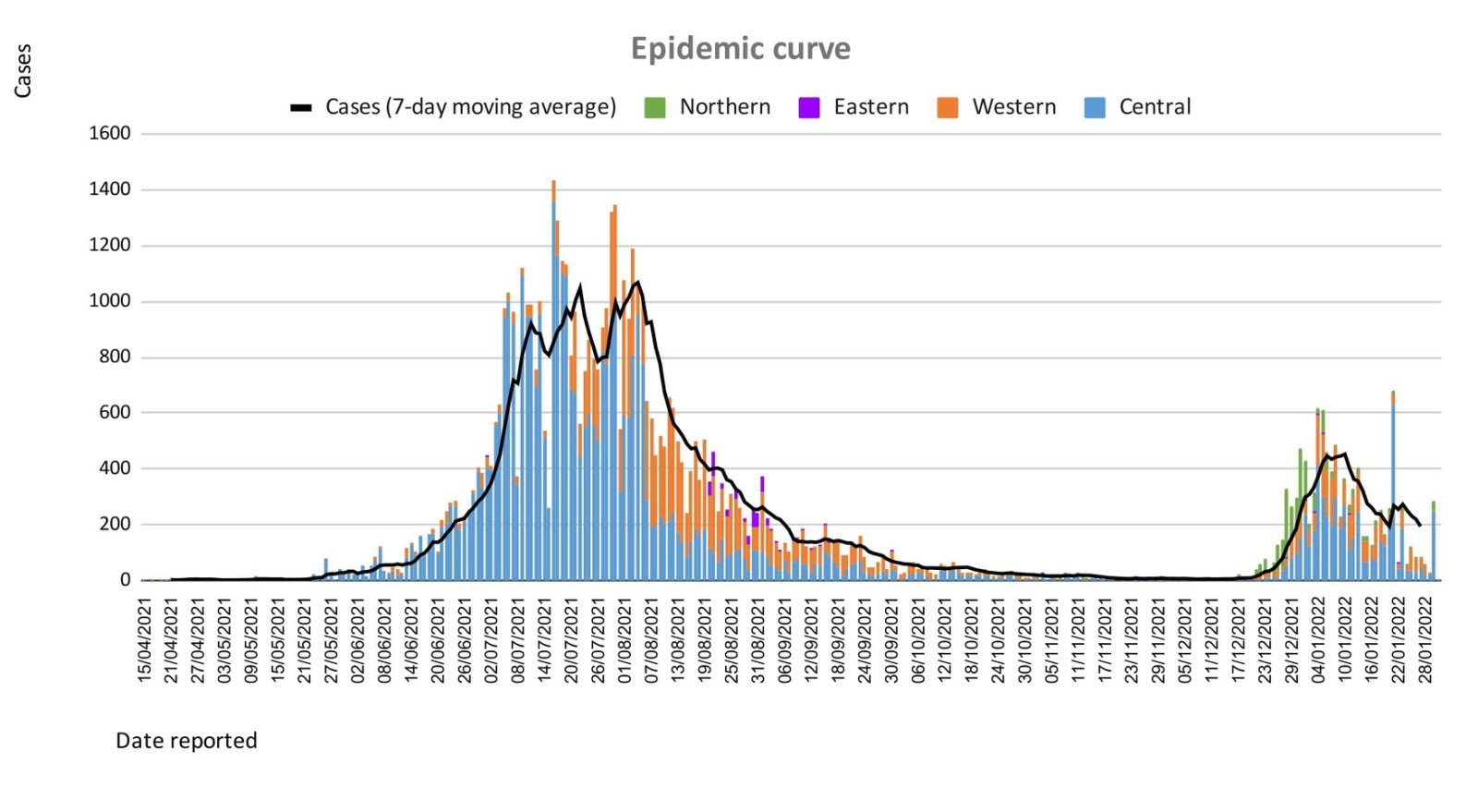
Since the last update, we have recorded 460 new cases of which 71 new cases were recorded on 29/01/2022; 54 new cases were recorded on 30/01/2022 and 335 new cases in the last 24 hours ending at 8 am this morning. Of the 460 cases recorded, 345 cases were in the Central Division; 71 cases in the Western Division, 43 cases in the Northern Division, and 1 case in the Eastern Division. Overall, there have been 62,785 cases recorded, with 68% of the cases from the Central Division, 28% of the cases from the Western Division, 1% of the cases from the Eastern Division, and 3% from the Northern Division. The national 7-day rolling average of cases as of 27th January is 194 daily cases. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
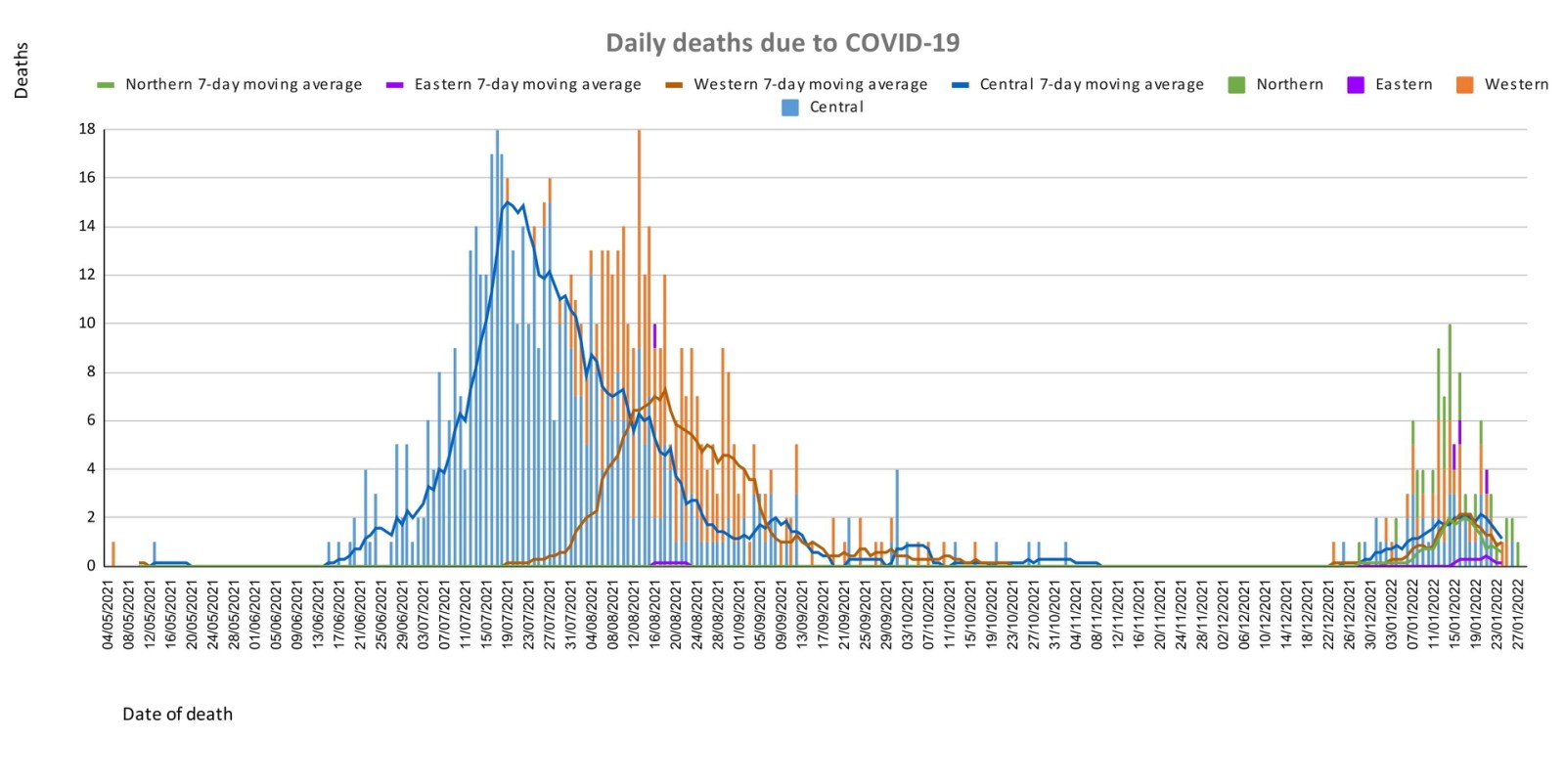
| Deaths:
Analysis of Deaths in the Third Wave Table 1: Death rates by Division
An analysis of the 105 deaths recorded in the third wave show that, while the Central Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population.(Note: There are deaths currently being investigated from the Western Division for the same time period, therefore the rate for that division may increase). Table 2: Deaths by Age Group
For the 105 deaths in the third wave, the rates of death when adjusted for population, have been highest in the age groups 50 and upwards. The 5 deaths from the under 19 age group were in children with significant underlying medical conditions. Table 3: Deaths by Vaccination Status
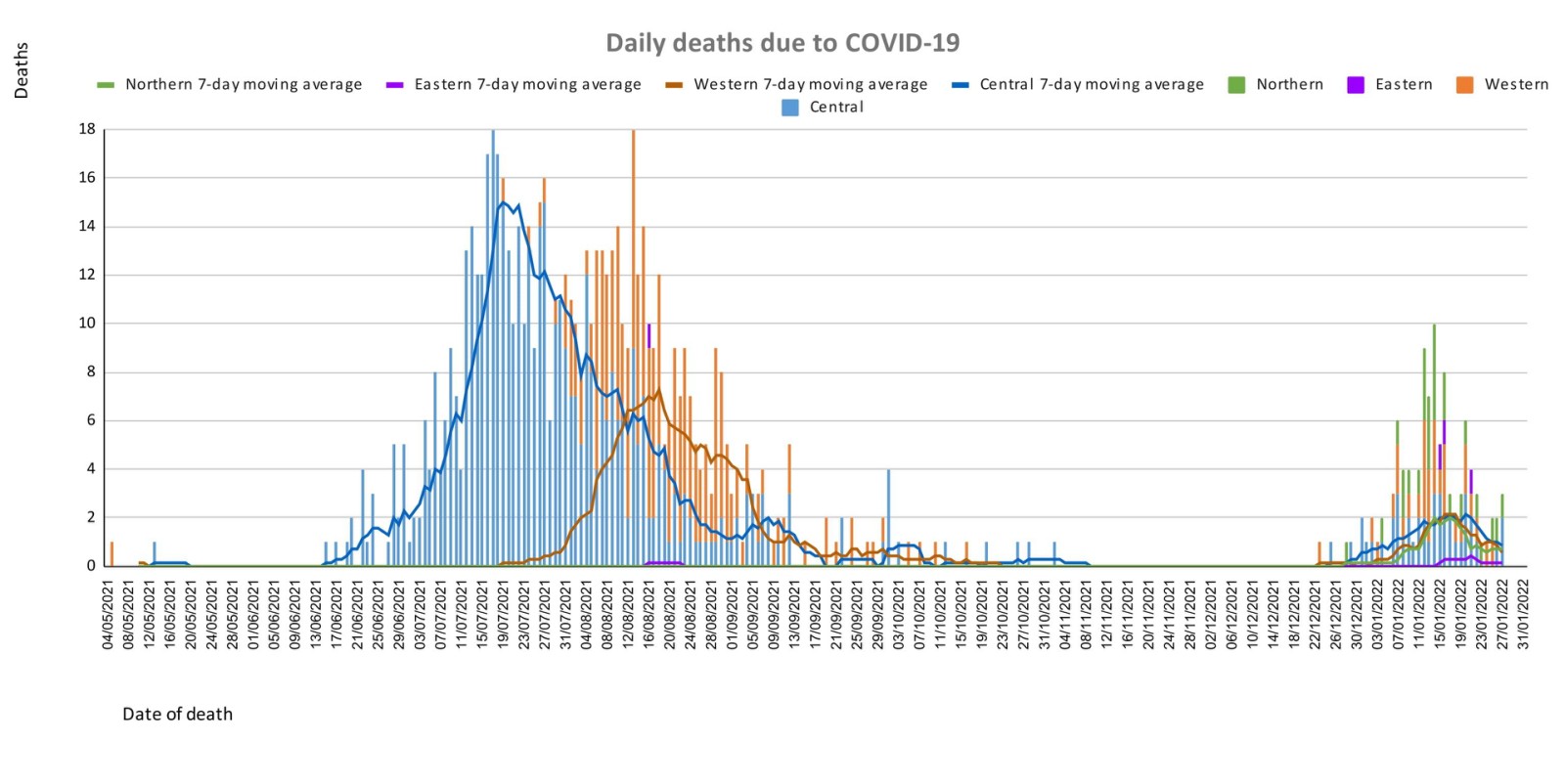
Out of 105 COVID -19 deaths reported in the third wave, three deaths were in the population not eligible for vaccination (under age 12). An analysis was done for the 102 deaths in the vaccine-eligible population. When adjusted for population in the fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we can see that death rates per 100,000 population are 7.1 deaths per 100,000 for fully vaccinated adults and 130.9 deaths per 100,000 for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying from COVID-19 at a rate 18.4 times higher than fully vaccinated adults during this current wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no deaths in individuals who received a booster (3rd dose) of the vaccine. New deaths to report There are 3 new COVID-19 deaths to report from 27th to 28th January 2022. The first COVID-19 death to report is of a 92-year old female from the Central Division, who died at home on 27/01/2022. She was not vaccinated. The second COVID-19 death to report is of a 46-year old female from the Western Division, who died at home on 27/01/2022. She had significant pre-existing comorbidities and was not vaccinated. The third COVID-19 death to report is of a 79-year old female from the Central Division, who died at home on 28/01/2022. She had congenital comorbidity and was not vaccinated. There has been a total of 801 deaths due to COVID-19 in Fiji. Please note that due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported. Therefore, as of January 20th, 2022, the national 7 days rolling average for COVID-19 deaths per day is 2.9, with a case fatality rate of 1.32%. We have recorded 839 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
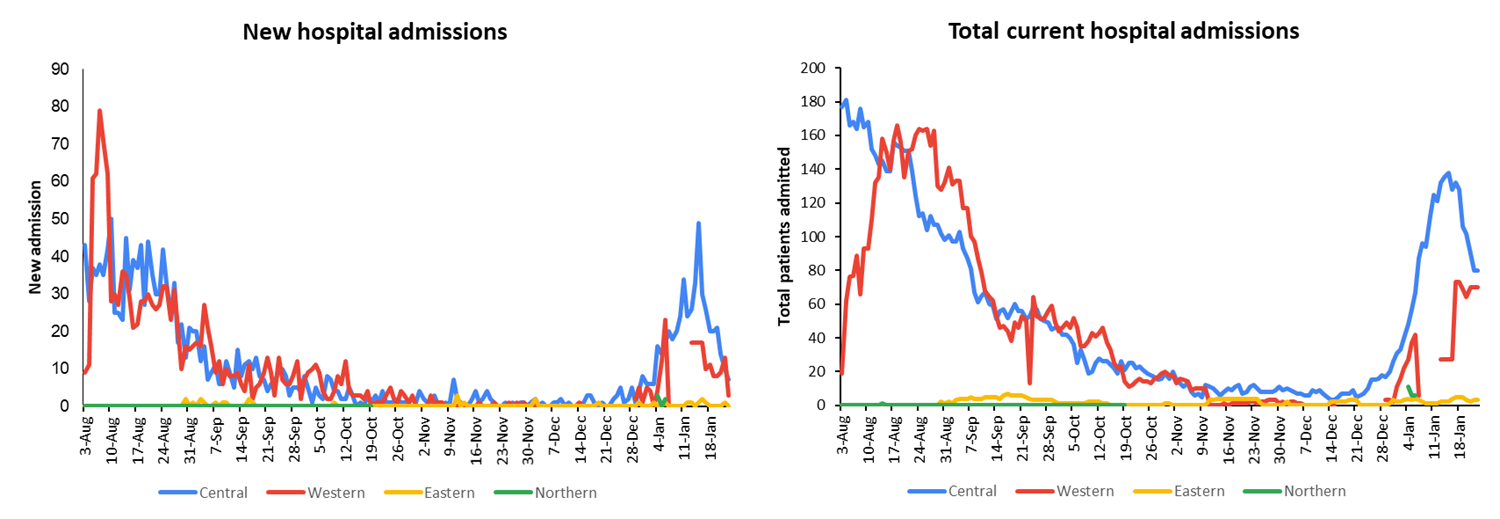
| Hospitalization:
There is a downward trend in daily hospitalisations. Using the WHO clinical severity classification, a greater percentage, 58% (n=58) of the admissions of COVID-19 positive patients are categorized as asymptomatic and mild,18% (n=18) are categorized as moderate and 22% (n=22) as severe with 2 cases in the critical category. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community. The number of people being admitted because of COVID-19 remains low. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Testing:
749 tests have been reported for January 30th, 2022. Total cumulative tests since 2020 is 492,136 tests. The 7-day daily test average is 302 tests per day or 0.3 tests per 1,000 population. The national 7-day average daily test positivity is 37.6%. The high positivity rate is an indication of widespread community transmission. |
Public Advisory:
Since my press statement of Friday, 28th January 2022, the hospital admissions data and informal employment data continue to indicate a downward trend in transmission. The death reports generated reflect delays not only in reporting but also in transmission as many of the deaths have occurred in a population that was not mobile.
The initial and subsequent analysis of the deaths in the vaccine-eligible population during this third wave has revealed that fully vaccinated adults have a 16.2 times lower rate of death from COVID-19 than unvaccinated adults. This is comparable to rates seen overseas, which is an indication of the quality of our COVID-19 vaccination program, even with the urgency of ensuring rapid deployment of vaccines in a very short time period. A testament to the work put in by our dedicated health teams and partner agencies to ensure that protocols are followed, and vaccines are administered properly to the people of Fiji. The huge difference in death rates between vaccinated and unvaccinated adults is even further evidence that vaccination lowers the risk of severe disease outcomes from COVID-19.
We have also highlighted how severe comorbidities and poor health-seeking behaviour have vastly contributed to severe outcomes. There has also been comprehensive global data to indicate that COVID 19 will remain endemic and as such will persist as a danger to the unvaccinated, those with severe comorbidities, and those in need of support to engage in better health-seeking behaviour.
All this indicates a need for a national reset for our national discourse on the health of our people. We need a new focus, from the media and members of the public, on chronic disease (especially NCDs) and health-seeking behaviour.
This speaks to 3 distinct strategies to facilitate resilience:
- Prevention of preventable chronic diseases of which NCDs are the most prominent
- Better control of controllable chronic diseases of which NCDs are the most prominent
- The promotion of better health-seeking behaviour
We will also need to urgently review and strengthen our public health measures to find, stop and prevent health threats wherever they arise. Much of this will depend on a coordinated effort to detect these health threats early, investigate and put in control measures early. The Medical Subdivisional Teams have been reminded to review and strengthen their community surveillance program and line list management of vulnerable persons.
However, the impact of these efforts cannot be sustained unless we get a broad level of support from the community in implementing the 3 strategies alluded to above and at the same time reduce the transmission of COVID-19 to protect our vulnerable populations. Maintaining the Vaccine Plus approach remains critical.
Vaccination
The booster dose program began at the end of November 2021. As of January 31st, 73,630 individuals have so far received booster doses of the Moderna COVID-19 vaccine from the 142, 240 persons considered eligible. This represents a 52% coverage rate for booster-eligible persons. We are also expecting to receive more Pfizer vaccines this week to be used for booster doses and as a vaccine for children. The booster vaccine and vaccination for children are not considered mandatory, however, we encourage all eligible individuals to be vaccinated or get a booster dose, and help navigate Fiji into a safer covid zone that supports the socio-economic revival and safer reopening of schools.
Vaccination of children under 12 years remains part of ongoing discussions as sourcing them remains difficult.