The Permanent Secretary for Health and Medical Services Dr. James Fong launched the revised Fiji IPC guidelines to further strengthen the health system and improve health care services in Fiji through the implementation of IPC measures in combating infectious diseases.
Together with the Launch he also opened the two-day training for IPCO officers from the health facilities in the Central Division including the staff at CWM.
While opening the two-day training Dr. Fong said as a follow-up to the training the team will be able to put together an IPC development plan that will link up the Public Health and Hospital Acute Networks to facilitate patient care.
“Infection prevention and control is an integral part of a health care system, one that needs to be implemented and recognised as a means of improving the quality of provision of health care together with, at the same time, providing a safe working environment for all healthcare professionals”, he added.
Effective IPC requires constant action at all levels of the health system, including policymakers, facility managers, health workers, and those who access health services.
The launching of the Fijian IPC Guideline today is indeed a Milestone for Fiji.
The Ministry acknowledges the contribution of the Pacific Community (SPC) through its Pacific Surveillance Network which has enabled us to Review and Develop the Fiji IPC that was developed in 2004 and the World Bank for their continued financial support.
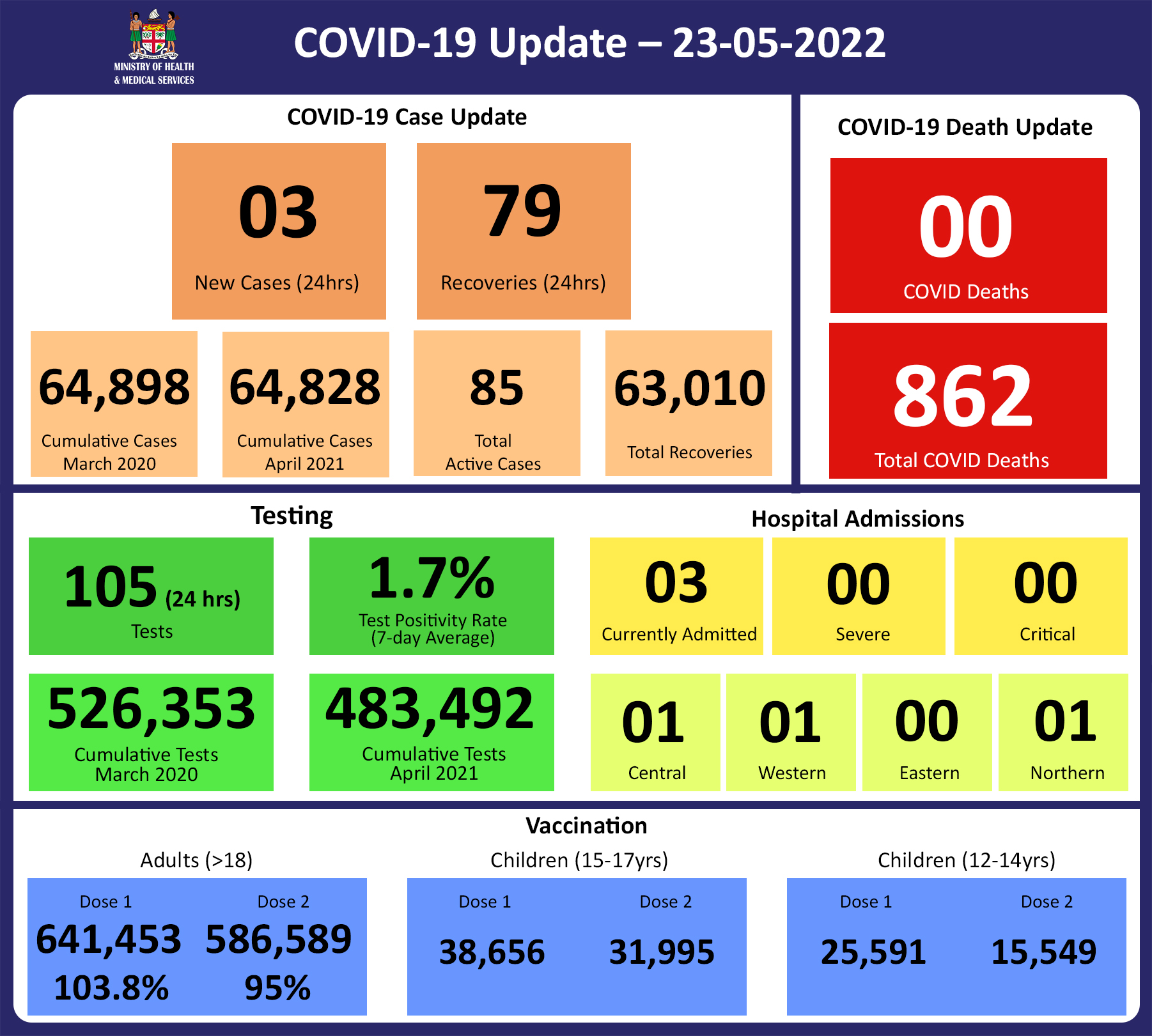
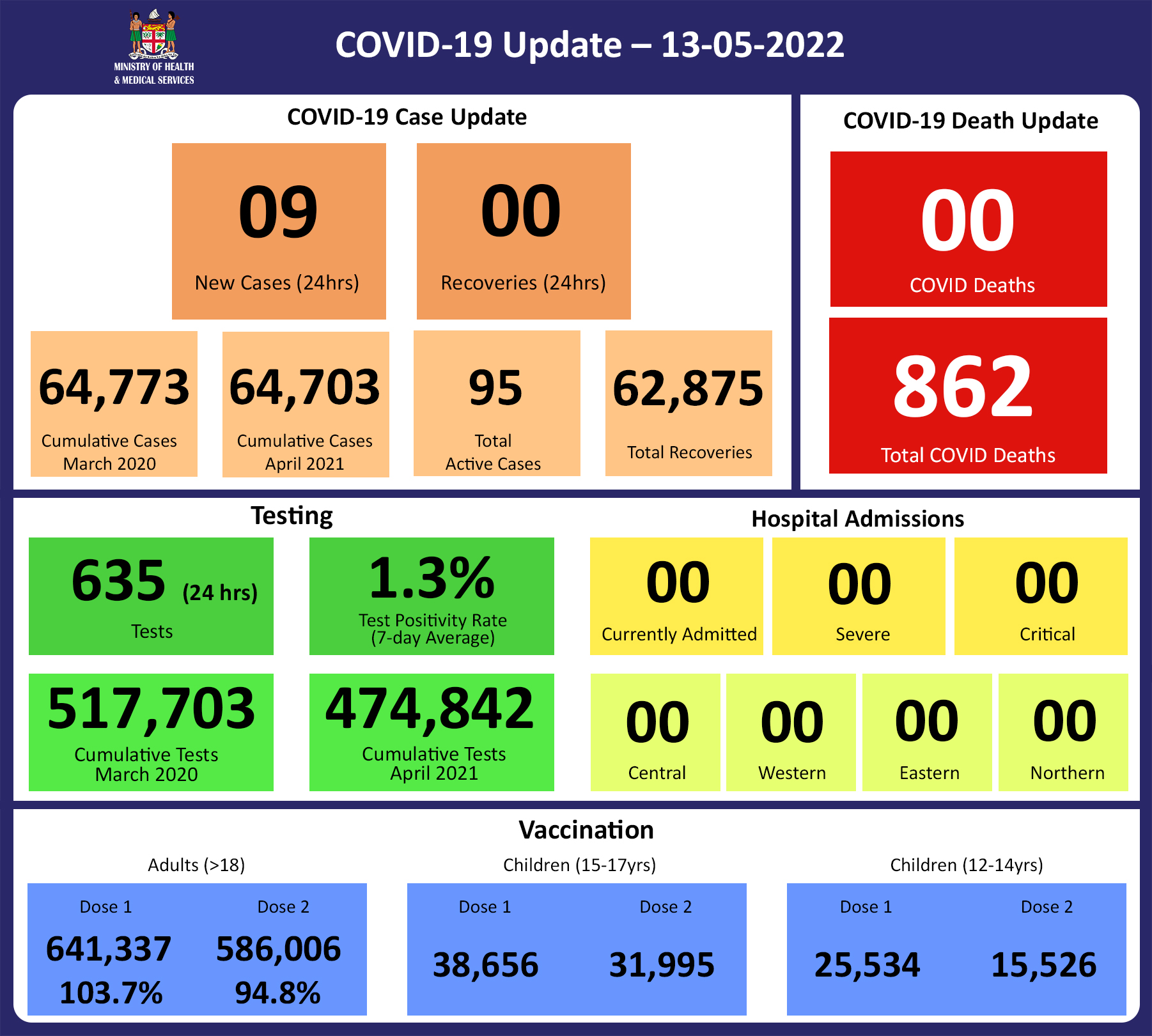
Since the last update, we have recorded 57 new cases of which 32 new cases were recorded on 20/05/2022; 7 new cases were recorded on 21/05/2022; 15 new cases were recorded on 22/05/2022 and 3 new cases in the last 24 hours ending at 8 am this morning.
Of the 57 cases recorded, 20 cases were recorded in the Central Division; 33 cases were recorded in the Western Division; 4 cases were recorded in the Northern and nil cases were recorded in the Eastern Division.
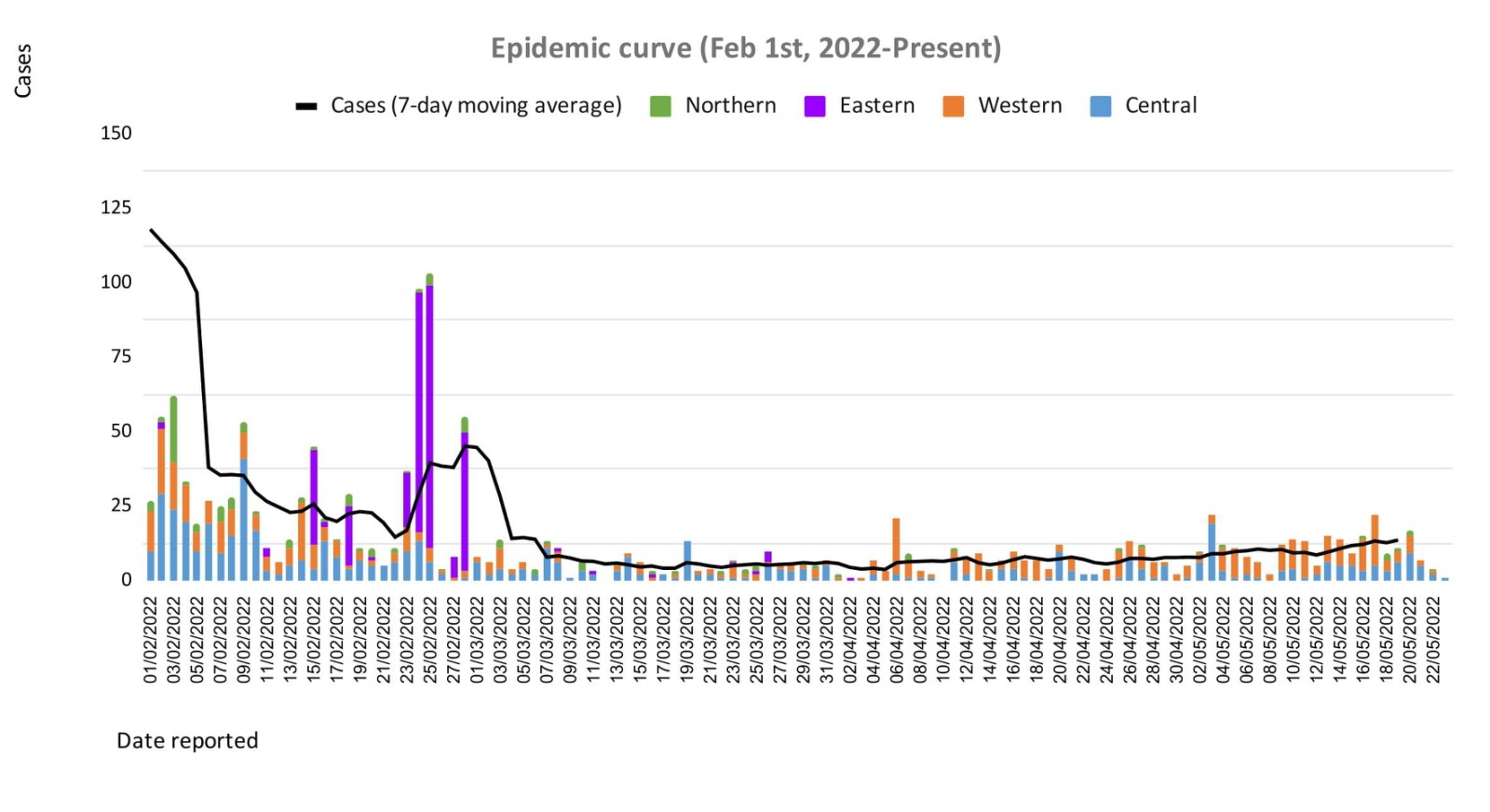
The national 7-day rolling average of cases as of 19th May is 14 daily cases.
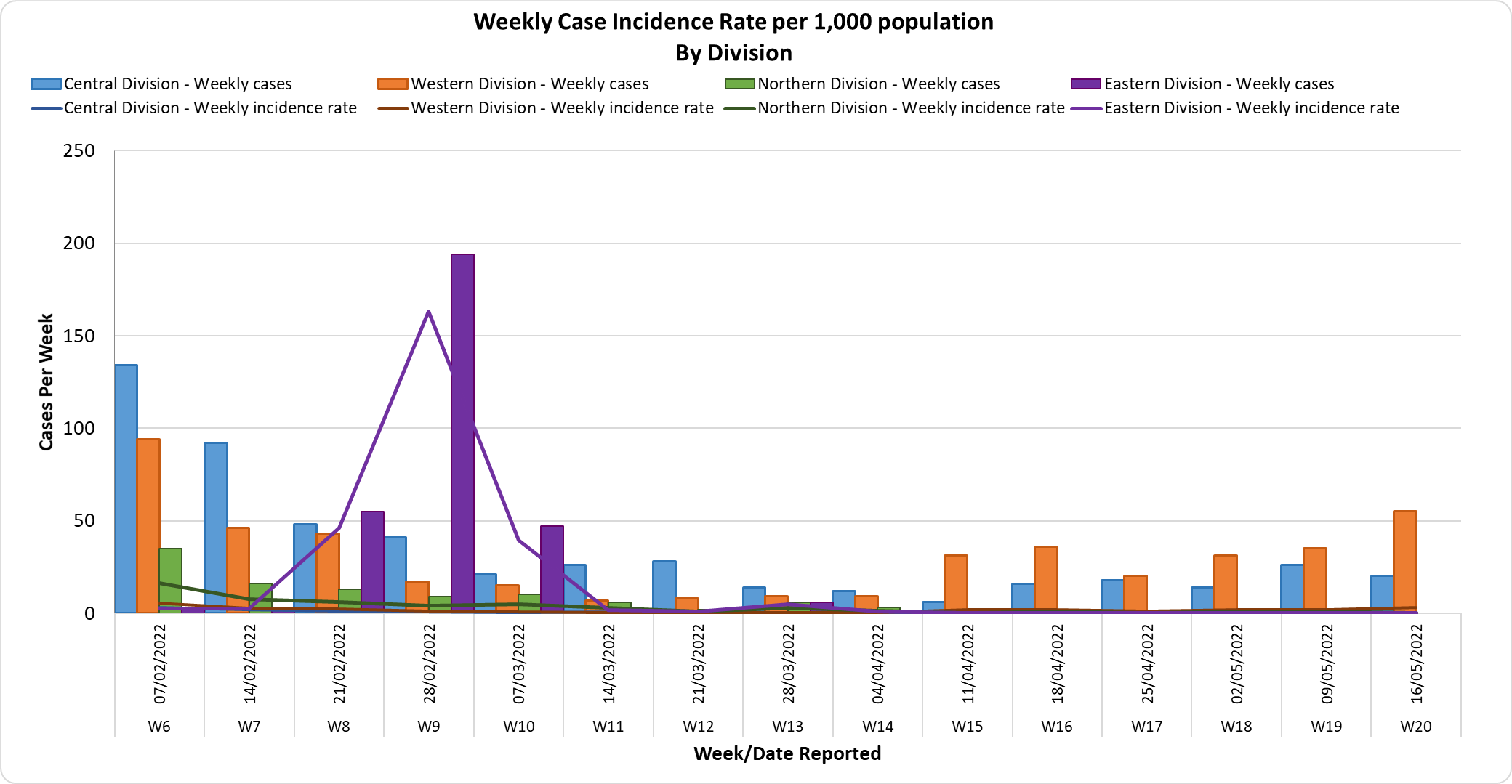
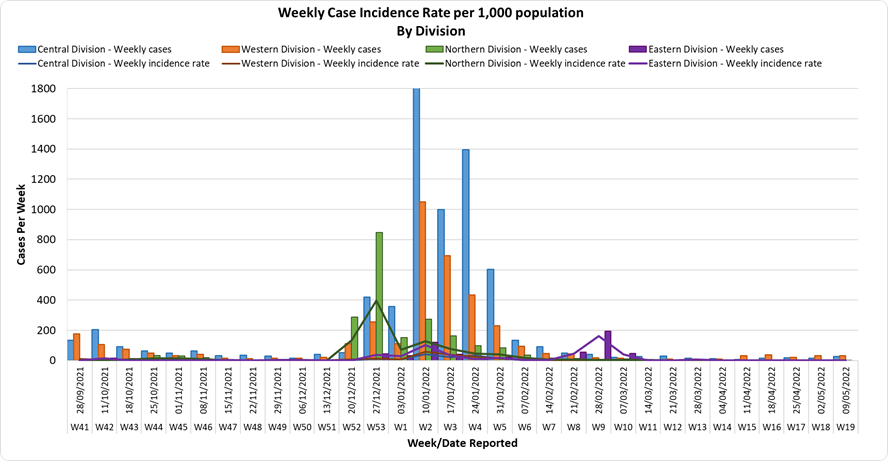
The Central Division cases constitute 67% of the cumulative total cases nationally, with the Western division making up 28%, 3% in the Northern Division, and 2% in the Eastern Division.
Deaths:
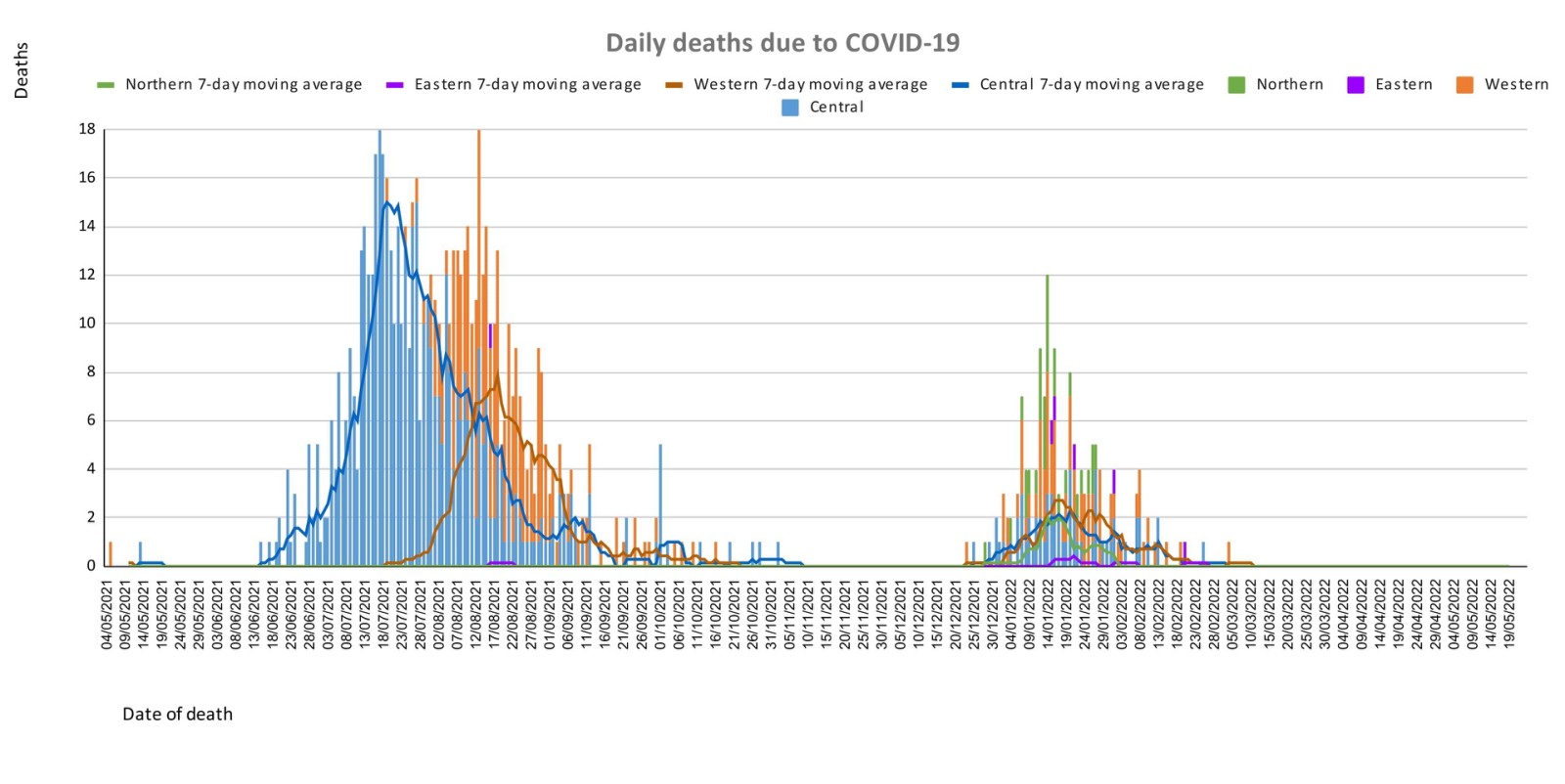
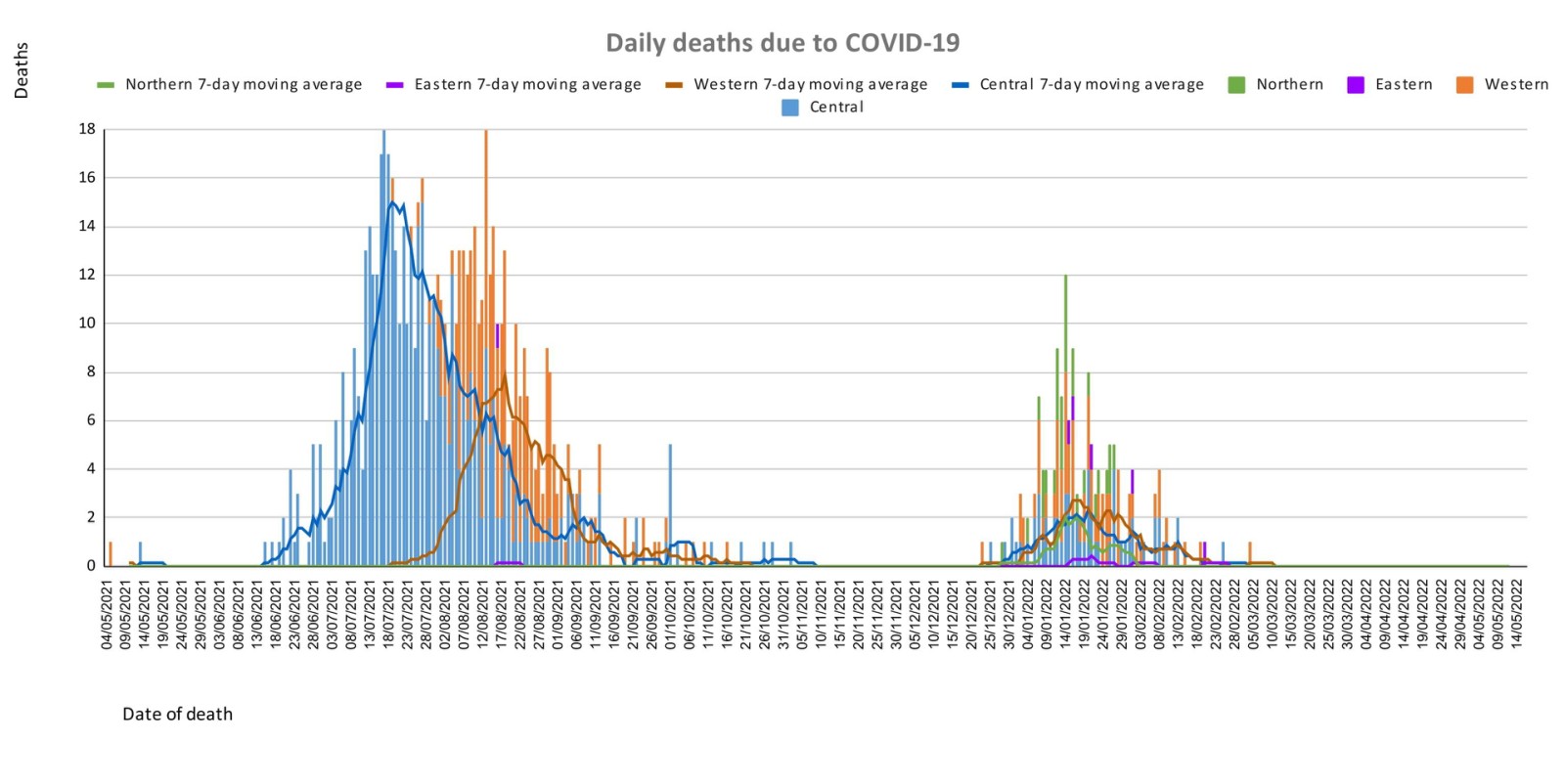
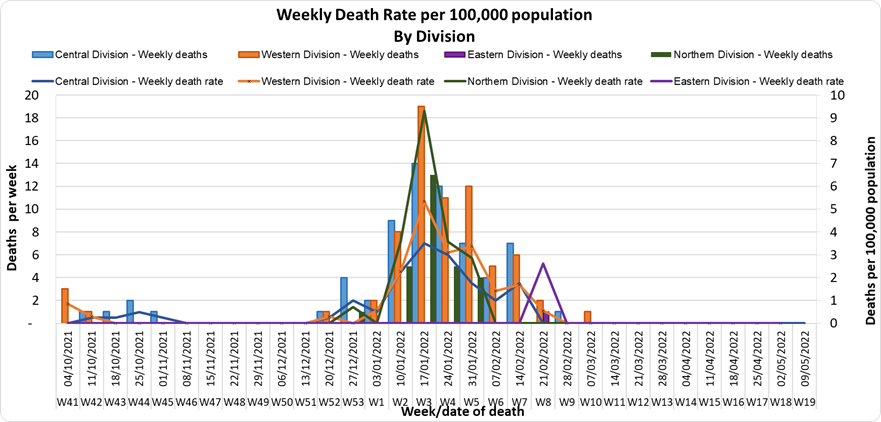
The curve depicts daily COVID-19 deaths by division since May 2021. It indicates a surge from last December, with peaks in mid-January 2022 followed by a downward trend, with the most recent death occurring on March 4th, 2022.
Analysis of Deaths in the Third Wave
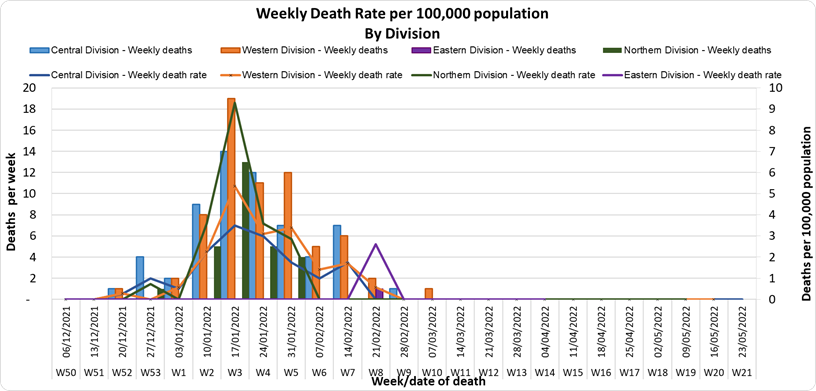
Table 1: Death rates by Division
Division
Total COVID Deaths
Deaths per 100,000
Central
61
15.4
Western
67
18.8
Northern
28
20.0
Eastern
5
13.0
An analysis of the 161 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population.
Table 2: Deaths by Age Group
Age Group
Total Deaths
Deaths per 100,000
population
0 – 9
6
3.3
10-19
2
1.3
20-29
3
2.1
30-39
4
2.9
40-49
6
5.4
50-59
21
23.1
60-69
33
63.5
70-79
50
223.2
80-89
28
497.6
90-99
6
1153.8
For the 161 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition.
Table 3: Deaths by Vaccination Status
Age Cohort
Total COVID deaths
Total Vaccinated/ Unvaccinated
Deaths per 100,000 Vaccinated Population
Deaths per 100,000 Unvaccinated Population
>18
129
59/94
10.1
275.2
15-17
1
0/1
0
6.6
12-14
1
0/1
0
2.5
Out of 161 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 161 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.1 per 100,000 population for fully vaccinated adults and 275.2 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 27.2 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine.
There have been a total of 862 deaths due to COVID-19 in Fiji. As of April 24th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported.
We have also recorded 939 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths.
Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, there are 67% (n=2) cases in the asymptomatic and mild category, 33% (n=1) are categorized as severe and nil cases in the moderate and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community.
Testing:
105 tests have been reported for May 22nd, 2022. Total cumulative tests since 2020 are 526,353 tests. The 7-day daily test average is 827 tests per day or 0.9 tests per 1,000 population.
The national 7-day average daily test positivity is 1.7%, which is within the WHO recommendation of 5%.
Public Advisory
COVID-19 trends
We have noted an increasing trend in cases. While the increase is not obvious on our epidemiological curve graph we are maintaining close surveillance of case numbers. We are monitoring hospital admissions and testing for COVID-19. As indicated above while our admissions for COVID-19 remain low, this is an indicator that remains important to our ongoing response plans. The case trends do highlight the need to escalate our booster dose coverage.
International communicable disease outbreaks
AS previously mentioned, the Ministry’s Fiji Centre for Disease Control (Fiji CDC) and Border Health Protection Unit (BHPU) are monitoring international outbreaks of concern, which include Ebola Virus Disease in the Democratic Republic of Congo, Japanese Encephalitis in Australia, acute hepatitis of unknown origin in multiple countries, and monkeypox in the United Kingdom and other countries. Where appropriate, specific interventions have been put in place or strengthened in response. The situation will continue to be monitored, assessed, and responded to based on the available scientific evidence, best practice, and advice from expert authorities.
Monkeypox
As we continue our recovery path during this pandemic, the strategies for resilience require urgent and early preparedness and response planning against any potential threat.
Monkeypox is a rare disease that is caused by infection with the monkeypox virus. It is endemic to certain countries in Central and Western Africa, and the causative virus is of the same family as the smallpox virus. Monkeypox outbreaks have been recently reported in a growing number of countries that are not endemic for the disease, including the United Kingdom, Spain, Portugal, France, Italy, Germany, Sweden, the Netherlands Canada, the United States of America, and Australia.
Monkeypox is usually a self-limiting illness, which means that most people recover with just supportive treatment within several weeks. However, severe illness can occur in some individuals. It does not spread easily between people but person to person transmission may occur through:
contact with clothing or linens (such as bedding or towels) used by an infected person
direct contact with monkeypox skin lesions or scabs
exposure to respiratory droplets eg through coughing or sneezing
The Ministry is working with communications and community engagement teams on appropriate public advisories. We need to arm ourselves with the knowledge to protect ourselves to reduce the chances of spread in our community. Infection prevention protocols are currently being put together at the border and in community facilities. One key focus will be to ensure we have the ability to maintain oversight over travellers from selected countries to ensure early diagnosis, treatment, and contact tracing.
Overall symptoms of the virus can include:
fever, chills, muscle aches, backache, swollen lymph nodes, and exhaustion
an unusual rash, which typically starts on the face, then may spread elsewhere on the body.
All doctors and Nurses in the community need to ensure they are well informed of how cases present and be vigilant in helping to ensure cases are diagnosed early.
Prevention of transmission of infection by respiratory and contact routes is required. Appropriate respiratory isolation is essential for suspected and confirmed cases. Scabs are also infectious and care must be taken to avoid infection by handling bedding, clothing, and so on. Workplaces especially in key sectors will be asked to escalate their Infection Prevention and Control and ensure practices are maintained.
The major priority for the Ministry of Health and Medical Services is to have a response plan that will include surveillance with rapid response and containment protocols and at the same time have a minimal social and economic impact. A key focus will be on ensuring that those suspected or confirmed to have monkeypox must be able to be managed in a dignified manner with no threat of stigmatization. Each citizen’s duty to contribute to protecting Fiji must be the priority.
We are in discussions with our reference laboratory in Melbourne to ensure access to definitive tests. Our ongoing efforts to have genomic sequencing capability in the Fiji CDC will provide us with greater capacity to deal with infection threats now and in the future.
We are also in discussions with WHO to ensure we preposition access to vaccines and medications used to treat monkeypox.
It is important however to ensure that in escalating community-wide infection prevention and control measures we are responding to current threats and creating communitywide resilience to upcoming threats. Our ongoing engagement in a healthy lifestyle to mitigate NCDs is also part of the overall focus on building back better and stronger.
The Ministry of Health and Medical Services will be disseminating more specific advisories over the next few days to weeks. Further updated knowledge about the monkeypox virus will be shared as they are known.
Ongoing Medical Recovery Efforts
With the reduction in COVID-19 cases and in people presenting to health centres with acute respiratory illness, the MOHMS team is better positioned to focus more on health facilities and health care provision capabilities to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment.
Our command centres and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and to work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
We are also focused on carrying out general health service work more efficiently in all facilities, and a key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is a strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities and allow for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision-making and action within the Ministry.
COVID-19 Vaccination
As of the 23rd of May, a total of 127,951 individuals have so far received booster doses. This represents 29.5% of those eligible for a booster dose. The booster dose interval for eligible persons has been reduced to 3 months from the 2nd dose. This is in recognition of the risk of disease surge based on waning 2 doses covid vaccine protection, slow booster uptake, increased international travel with the relaxation of border measures, and ongoing outbreaks in various parts of the world. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The public is urged to get booster vaccine doses, and the list of vaccination sites is provided daily on the MOH. We have accepted an offer of 50,000 doses of Pfizer paediatric doses for children aged 5 to 11 by the Aotearoa New Zealand Government. Our vaccination team is currently discussing with counterparts in NZ on further details while our efforts to source more through our other development partners are ongoing.
Our school vaccination program has also been progressing such that with the 95% adult coverage rate, 90.6% of all persons over 12 years have had 2 doses of the COVID-19 vaccine.
We will continue to monitor the evidence on post-infection immunity based on quality data generated globally. However, until we have a better sense of the role of post-infection immunity, the Ministry of Health will continue to define our level of protection based on vaccination numbers
Given the current stocks of Pfizer vaccines, we are now covering the Primary doses for those yet to be vaccinated and for Dose 2 if individuals were vaccinated with either Moderna or Astra Zeneca while the 12-14-year-olds continue with the Pfizer vaccine. The new supplies of MODERNA are expected to be available in-country at the end of the month.
Cold and flu
The Ministry of Health and Medical Services has noted an increase in people becoming ill with cold and flu-like illnesses as we are coming into our dry and cold season. This increase is especially seen in infants and children under the age of 5. The paediatrics department at CWM Hospital is also seeing an increase in children under the age of 5, especially infants, being admitted with acute respiratory illnesses while testing negative for COVID-19 and influenza. It has been expected that as restrictions intended to prevent transmission of COVID-19 were lifted (including mandatory masking, physical distancing, and school and border closures) other respiratory viruses that normally circulate would begin to re-emerge similar to pre-COVID levels, and possibly even at higher levels due to a decrease in population immunity to seasonal viruses, as cold/flu cases were low during the last two years.
Since the last update, we have recorded 29 new cases of which 4 new cases were recorded on 17/05/2022; 8 new cases were recorded on 18/05/2022 and 17 new cases in the last 24 hours ending at 8 am this morning.
Of the 29 cases recorded, 14 cases were recorded in the Central Division; 13 cases were recorded in the Western Division; 2 cases were recorded in the Northern Division and nil cases were recorded in the Eastern Division.
The national 7-day rolling average of cases as of 15th May is 12 daily cases.
In the 7 days until 18/05/2022, 28 new cases were recorded in the Central division, 26 new cases in the Western division, 1 new case in the Northern Division and nil new cases in the Eastern Division.
The Central Division cases constitute 67% of the cumulative total cases nationally, with the Western division making up 28%, 3% in the Northern Division, and 2% in the Eastern Division.
Deaths:The curve depicts daily COVID-19 deaths by division since May 2021. It indicates a surge from last December, with peaks in mid-January 2022 followed by a downward trend, with the most recent death occurring on March 4th, 2022.
There is no COVID-19 death to report today.
Analysis of Deaths in the Third Wave
Table 1: Death rates by Division
Division
Total COVID Deaths
Deaths per 100,000
Central
61
15.4
Western
67
18.8
Northern
28
20.0
Eastern
5
13.0
An analysis of the 161 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population.
Table 2: Deaths by Age Group
Age Group
Total Deaths
Deaths per 100,000
population
0 – 9
6
3.3
10-19
2
1.3
20-29
3
2.1
30-39
4
2.9
40-49
6
5.4
50-59
21
23.1
60-69
33
63.5
70-79
50
223.2
80-89
28
497.6
90-99
6
1153.8
For the 161 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition.
Table 3: Deaths by Vaccination Status
Age Cohort
Total COVID deaths
Total Vaccinated/ Unvaccinated
Deaths per 100,000 Vaccinated Population
Deaths per 100,000 Unvaccinated Population
>18
129
59/94
10.1
275.2
15-17
1
0/1
0
6.6
12-14
1
0/1
0
2.5
Out of 161 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 161 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.1 per 100,000 population for fully vaccinated adults and 275.2 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 27.2 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine.
There have been a total of 862 deaths due to COVID-19 in Fiji. As of April 24th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported.
We have also recorded 939 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths.
Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, there are 50% (n=1) cases in the asymptomatic and mild categories, and 50% (n=1) are categorized as moderate and nil cases in the severe and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community.
Testing:
156 tests have been reported for May 18th, 2022. Total cumulative tests since 2020 are 520,908 tests. The 7-day daily test average is 548 tests per day or 0.6 tests per 1,000 population.
The national 7-day average daily test positivity is 4.6%, which is within the WHO recommendation of 5%.
Public Advisory
Engaging COVID safety without mandates or quarantine
Since the 7th of April and the lifting of our quarantine measures and increased international travel, our community, and border surveillance screening data continue to report a low positivity rate despite the ongoing pandemic, and the continued evolution of Omicron variants. While there is a low positivity rate among arrivals we are seeing positive arrivals. We are also aware that a key aspect of living with Covid is to have a strong community surveillance system within the community AND at the border. This will allow early identification of community outbreaks and facilitate early response. Early response capability is a key part of mitigating the risk of severe disease and severe containment measures and to further easing pre-departure conditions for international travel. As part of our community surveillance exercise, we will be transitioning to t9he more routine use of throat and nasal swabs as opposed to the more uncomfortable nasopharyngeal swabs
The Ministry informs the public that for the positive cases among arrivals, existing protocols have been instituted to ensure travellers that return positive COVID-19 test results follow protocols and isolate for the required 7 – days as advised.
However, the Ministry is concerned that there are travellers who are not adhering to the 7-days of isolation and continue to be mobile during that 7-day isolation period.
We call on the public to support the protection and safety of all Fijians by reminding travellers from overseas who are visiting friends and relatives of the importance of isolating themselves for 7 days if they test positive for COVID-19. As a nation, Fiji has emerged from the period of restrictions that were instituted to protect our people and our country from COVID-19. We need not be reminded of the high number of positive cases and the number of deaths from COVID-19. The Ministry reiterates that the lifting of masking and other mandates and easing of travel restrictions is NOT a sign that the risk of outbreak and resurgence of COVID-19 is over. It is important that we continue to work together to protect ourselves, our communities, and our country from any further
The following prevention measures continue; the promotion of vaccination, personal COVID-safe hygiene habits, and workplace ventilation and air cleaning measures. We recommend everyone continue to employ COVID-safe measures to prevent infection and the spread of infection: Frequently wash your hands or use an alcohol-based hand sanitizer, stay home if you feel sick, cover your mouth and nose with a tissue or the bend of your elbow if you cough or sneeze, wear a mask if you have any signs of a respiratory illness.
We have dropped the pre-departure testing requirement for travellers coming into Fiji and also we now require international arrivals to test within 72 hours of arrival. Beyond this potential change, our border protection will be mediated by the fact that all travellers over 16 years are vaccinated. Inbound travellers aged 12 years and above must produce proof of a pre-booked and pre-paid rapid antigen test, to be administered within 72 hours of arrival in Fiji. Booking for tests can be made through this link: https://entrytestfiji.com. There will be exemptions for those who have tested positive and recovered from COVID-19 within the 30 days before travel and have fit-to-fly certificates. Failure to comply with arrival testing once in Fiji will result in a spot fine of $1000.
Ongoing Medical Recovery Efforts
With the reduction in COVID-19 cases and in people presenting to health centres with acute respiratory illness, the MOHMS team is better positioned to focus more on health facilities and health care provision capabilities to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment.
Our command centres and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and to work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
We are also focused on carrying out general health service work more efficiently in all facilities, and a key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is a strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities and allow for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision-making and action within the Ministry.
COVID-19 Vaccination
As of the 19th of May, a total of 127,480 individuals have so far received booster doses. This represents 29.5% of those eligible for a booster dose. The booster dose interval for eligible persons has been reduced to 3 months from the 2nd dose. This is in recognition of the risk of disease surge based on waning 2 doses covid vaccine protection, slow booster uptake, increased international travel with the relaxation of border measures, and ongoing outbreaks in various parts of the world. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The public is urged to get booster vaccine doses, and the list of vaccination sites is provided daily on the MOH. We have accepted an offer of 50,000 doses of Pfizer paediatric doses for children aged 5 to 11 by the Aotearoa New Zealand Government. Our vaccination team is currently discussing with counterparts in NZ on further details while our efforts to source more through our other development partners are ongoing.
Our school vaccination program has also been progressing such that with the 95% adult coverage rate, 90.6% of all persons over 12 years have had 2 doses of the COVID-19 vaccine.
We will continue to monitor the evidence on post-infection immunity based on quality data generated globally. However, until we have a better sense of the role of post-infection immunity, the Ministry of Health will continue to define our level of protection based on vaccination numbers
Given the current stocks of Pfizer vaccines, we are now covering the Primary doses for those yet to be vaccinated and for Dose 2 if individuals were vaccinated with either Moderna or Astra Zeneca while the 12-14-year-olds continue with the Pfizer vaccine. The new supplies of MODERNA are expected to be available in-country at the end of the month.
Leptospirosis
The leptospirosis bacteria is spread to humans through the urine of infected animals, such as cows, pigs, rats, and dogs. To reduce your individual risk, it is important to understand that exposure to animals, soil, mud, and floodwaters during work or recreational activities increases your risk of infection.
Important prevention measures include wearing full covered footwear at all times when going outdoors, avoiding wading or swimming in flooded waters, using clean fresh water to wash up after exposure to muddy waters, and keeping all food and drinks covered and away from rats. For workplaces, practice good personal hygiene at all times, cover cuts and wounds well, and use protective equipment, especially footwear when in flooded and/or muddy areas.
We are also urging all parents and guardians to prevent children from playing in the mud or swimming in flooded rivers or creeks, and ensure that they wear shoes when outside.
Symptoms and treatment
Early treatment can decrease the severity and duration of the disease. Please seek medical care if you have recently had contact with floodwaters, mud, or animals, and develop the following symptoms: fever, muscle pain, or headache. You may also have red eyes, loss of appetite, nausea/vomiting, dizziness, or feel weak.
Leptospirosis can be treated with appropriate antibiotic medications prescribed by a doctor if treatment is sought early. Danger signs for severe leptospirosis include shortness of breath, coughing blood, chest pain, yellow eyes/skin (jaundice), signs of bleeding (including unexplained bruising), decreased or increased urination, and difficulty staying awake. Severe leptospirosis is life-threatening, and anyone with these symptoms must be taken to the hospital immediately.
Typhoid fever
Typhoid fever is typically found in areas that do not have access to proper toilet facilities and/or clean drinking water. We strongly encourage people who live in rural areas, informal urban areas, and any other areas where access to clean drinking water is limited, to boil all drinking water. We must all also continue to practice basic hygiene measures such as frequently washing hands with soap and water, especially after visiting the toilet and before eating or preparing food.
Dengue Fever
We continue to urge everyone to get rid of potential mosquito breeding places, such as empty containers inside and outside your homes that may collect water, including discarded tires, flower vases, and pot plant bases. Protect yourself from being bitten by mosquitoes by using mosquito screens in your home, and mosquito repellents.
Cold and flu
The Ministry of Health and Medical Services has noted an increase in people becoming ill with cold and flu-like illnesses as we are coming into our dry and cold season. This increase is especially seen in infants and children under the age of 5. The paediatrics department at CWM Hospital is also seeing an increase in children under the age of 5, especially infants, being admitted with acute respiratory illnesses while testing negative for COVID-19 and influenza. It has been expected that as restrictions intended to prevent transmission of COVID-19 were lifted (including mandatory masking, physical distancing, and school and border closures) other respiratory viruses that normally circulate would begin to re-emerge similar to pre-COVID levels, and possibly even at higher levels due to a decrease in population immunity to seasonal viruses, as cold/flu cases were low during the last two years.
Care for children with cold and flu symptoms
Keep your child hydrated to reduce cold and flu symptoms and help them feel better. Fevers can result in dehydration. Your child may not feel as thirsty as they normally would, and they may be uncomfortable when drinking, so it is important to encourage them to drink plenty of fluids like fresh fruit juices and water (e.g. lemon juice).
Dehydration can be very serious in babies, especially if they’re under 3 months old. Go immediately to your nearest health centre or doctor if you suspect your baby is dehydrated. Some signs may include:
no tears when crying
dry lips
a soft spot in the head that seems sunken-in
decreased activity
urinating less than three to four times in 24 hours
If your child is breastfed, attempt to breastfeed them more frequently than usual. Your baby may be less interested in breastfeeding if they’re sick. You may have to have several short feeding sessions or express breast milk and give in a small cup in order for them to consume enough fluid.
Clear up stuffed nasal passages and loosen mucous to ease cough
Careful use of a steam source in a closed room can help to relieve a stuffed nose and soften mucous to make coughing up mucous easier.
Saline drops for the nose can also be bought at pharmacies to soften nasal mucous and facilitate its discharge
Alternatively use a small amount of Vicks rub mixed with oil over the heels of feet for children >3 months old
If your child is over 1-year-old, try giving honey for a cough instead of medication. You can give 2 to 5 milliliters (mL) of honey a few times during the day.
Encourage rest
Extra rest can help your child recover faster.
Fever
Your child may be very hot due to fever. Dress them lightly and avoid heavy blankets or excessive layers that could make them feel hotter. A mild fever does not need treatment as fever is the body’s way of fighting off an infection. A lukewarm bath can also help them cool off and wind down before taking a nap or going to sleep for the night.
Seek medical care
Sometimes even the best at-home care isn’t enough to help your little one make a full recovery. Seek medical care right away if your child has any of the following:
has a fever greater than 38°C for more than two days, or a fever of 40°C or higher for any amount of time
has a fever of 38°C or higher and is under 3 months old
has a fever that doesn’t get better after taking Panadol
seems unusually drowsy or lethargic
won’t eat or drink
is wheezing or is short of breath
Prevention
After your child recovers, there are steps you can take to prevent cold and flu in the future. Wash all surfaces they came into contact with before or during their sickness. Encourage your children and other family members to wash their hands regularly to keep germs at bay.
Teach your child not to share food, drinks, or utensils when they eat. This assists in avoiding the spread of germs between them and their friends. Keep your child out of daycare or school when they are ill, especially if they have a fever. Keep them away from others with flu-like symptoms and avoid crowds.
International communicable disease outbreaks
The Ministry’s Fiji Centre for Disease Control (Fiji CDC) and Border Health Protection Unit (BHPU) are monitoring international outbreaks of concern, which include Ebola Virus Disease in the Democratic Republic of Congo, Japanese Encephalitis in Australia, acute hepatitis of unknown origin in multiple countries, and monkeypox in the United Kingdom and other countries. Where appropriate, specific interventions have been put in place or strengthened in response. The situation will continue to be monitored, assessed, and responded to based on the available scientific evidence, best practice, and advice from expert authorities.
Since the last update, we have recorded 39 new cases of which 0 new cases were recorded on 14/05/2022; 7 new cases were recorded on 15/05/2022 and 32 new cases in the last 24 hours ending at 8 am this morning.
Of the 39 cases recorded, 16 cases were recorded in the Central Division; 22 cases were recorded in the Western Division; 1 case was recorded in the Northern and nil cases were recorded in the Eastern Division.
The national 7-day rolling average of cases as of 12th May is 9 daily cases.
The Central Division cases constitute 67% of the cumulative total cases nationally, with the Western division making up 28%, 3% in the Northern Division, and 2% in the Eastern Division.
Deaths:The curve depicts daily COVID-19 deaths by division since May 2021. It indicates a surge from last December, with peaks in mid-January 2022 followed by a downward trend, with the most recent death occurring on March 4th 2022.
There is no COVID-19 death to report today.
Analysis of Deaths in the Third Wave
Table 1: Death rates by Division
Division
Total COVID Deaths
Deaths per 100,000
Central
61
15.4
Western
67
18.8
Northern
28
20.0
Eastern
5
13.0
An analysis of the 161 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population.
Table 2: Deaths by Age Group
Age Group
Total Deaths
Deaths per 100,000
population
0 – 9
6
3.3
10-19
2
1.3
20-29
3
2.1
30-39
4
2.9
40-49
6
5.4
50-59
21
23.1
60-69
33
63.5
70-79
50
223.2
80-89
28
497.6
90-99
6
1153.8
For the 161 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition.
Table 3: Deaths by Vaccination Status
Age Cohort
Total COVID deaths
Total Vaccinated/ Unvaccinated
Deaths per 100,000 Vaccinated Population
Deaths per 100,000 Unvaccinated Population
>18
129
59/94
10.1
275.2
15-17
1
0/1
0
6.6
12-14
1
0/1
0
2.5
Out of 161 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 161 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.1 per 100,000 population for fully vaccinated adults and 275.2 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 27.2 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine.
There have been a total of 862 deaths due to COVID-19 in Fiji. As of April 24th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported.
We have also recorded 939 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths.
Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, there are nil cases in the asymptomatic and mild, and 100% (n=1) are categorised as moderate and nil cases in the severe and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community.
Testing:
721 tests have been reported for May 15th, 2022. Total cumulative tests since 2020 are 520,560 tests. The 7-day daily test average is 854 tests per day or 1.0 tests per 1,000 population.
The national 7-day average daily test positivity is 2.0%, which is within the WHO recommendation of 5%.
Public Advisory
Engaging COVID safety without mandates or quarantine
Since the 7th of April and the lifting of our quarantine measures and increased international travel, our community and border surveillance screening data continue to report a low positivity rate despite the ongoing pandemic, and the continued evolution of Omicron variants. While there is a low positivity rate among arrivals we are seeing positive arrivals. We are also aware that a key aspect of living with Covid is to have a strong community surveillance system within the community AND at the border. This will allow early identification of community outbreaks and facilitate early response. Early response capability is a key part of mitigating the risk of severe disease and severe containment measures and to further easing pre-departure conditions for international travel. As part of our community surveillance exercise, we will be transitioning to t9he more routine use of throat and nasal swabs as opposed to the more uncomfortable nasopharyngeal swabs
The Ministry informs the public that for the positive cases among arrivals, existing protocols have been instituted to ensure travellers that return positive COVID-19 test results follow protocols and isolate for the required 7 – days as advised.
However, the Ministry is concerned that there are travellers who are not adhering to the 7-days of isolation and continue to be mobile during that 7-day isolation period.
We call on the public to support the protection and safety of all Fijians by reminding travellers from overseas who are visiting friends and relatives of the importance of isolating themselves for 7 days if they test positive for COVID-19. As a nation, Fiji has emerged from the period of restrictions that were instituted to protect our people and our country from COVID-19. We need not be reminded of the high number of positive cases and the number of deaths from COVID-19. The Ministry reiterates that the lifting of masking and other mandates and easing of travel restrictions is NOT a sign that the risk of outbreak and resurgence of COVID-19 is over. It is important that we continue to work together to protect ourselves, our communities and our country from any further
The following prevention measures continue; the promotion of vaccination, personal COVID-safe hygiene habits, and workplace ventilation and air cleaning measures. We recommend everyone continue to employ COVID-safe measures to prevent infection and the spread of infection: Frequently wash your hands or use an alcohol-based hand sanitiser, stay home if you feel sick, cover your mouth and nose with a tissue or the bend of your elbow if you cough or sneeze, wear a mask if you have any signs of a respiratory illness.
We have dropped the pre-departure testing requirement for travellers coming into Fiji and also we now require international arrivals to test within 72 hours of arrival. Beyond this potential change, our border protection will be mediated by the fact that all travellers over 16 years are vaccinated. Inbound travellers aged 12 years and above must produce proof of a pre-booked and pre-paid rapid antigen test, to be administered within 72 hours of arrival in Fiji. Booking for tests can be made through this link: https://entrytestfiji.com. There will be exemptions for those who have tested positive and recovered from COVID-19 within the 30 days before travel and have fit-to-fly certificates. Failure to comply with arrival testing once in Fiji will result in a spot fine of $1000.
Ongoing Medical Recovery Efforts
With the reduction in COVID-19 cases and in people presenting to health centres with acute respiratory illness, the MOHMS team is better positioned to focus more on health facilities and health care provision capabilities to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment.
Our command centres and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and to work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
We are also focused on carrying out general health service work more efficiently in all facilities, and a key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is a strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities and allow for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision making and action within the Ministry.
COVID-19 Vaccination
As of the 16th of May, a total of 126,926 individuals have so far received booster doses. This represents 29.5% of those eligible for a booster dose. The booster dose interval for eligible persons has been reduced to 3 months from the 2nd dose. This is in recognition of the risk of disease surge based on waning 2 doses covid vaccine protection, slow booster uptake, increased international travel with the relaxation of border measures, and ongoing outbreaks in various parts of the world. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The public is urged to get booster vaccine doses, and the list of vaccination sites is provided daily on the MOH. We have accepted an offer of 50,000 doses of Pfizer paediatric doses for children aged 5 to 11 by the Aotearoa New Zealand Government. Our vaccination team is currently discussing with counterparts in NZ on further details while our efforts to source more through our other development partners are ongoing.
Our school vaccination program has also been progressing such that with the 95% adult coverage rate, 90.6% of all persons over 12 years have had 2 doses of the COVID-19 vaccine.
We will continue to monitor the evidence on post-infection immunity based on quality data generated globally. However, until we have a better sense of the role of post-infection immunity, the Ministry of Health will continue to define our level of protection based on vaccination numbers
Given the current stocks of Pfizer vaccines, we are now covering the Primary doses for those yet to be vaccinated and for Dose 2 if individuals were vaccinated with either Moderna or Astra Zeneca while the 12-14-year-olds continue with the Pfizer vaccine. The new supplies of MODERNA are expected to be available in-country at the end of the month.
Leptospirosis
There have been 2068 lab-confirmed cases of leptospirosis this year, with 111 new cases to report since the last update. A slight upward trend in cases with case numbers is noted above the outbreak threshold nationally, driven by cases in the Western Division. Case numbers are above the expected numbers for this time of the year.
Case numbers in the Western Division are increasing and remain above the outbreak alert threshold, indicating more cases than the expected number for this time of the year for this endemic disease. In the West, there have been 864 lab-confirmed cases, with 54 new cases since the last update.
In the Central Division, there have been 715 cases, with 29 new cases since the last update. Case numbers have increased towards the outbreak alert threshold in the last two weeks in Central..
In the Northern Division, there have been 427 cases, with 27 new cases since the last update. Case numbers have risen above the outbreak alert threshold in the last week, and are just above the average number of cases expected at this time of the year.
In the Eastern Division, there have been 62 cases, with 1 new case reported since the last update. Case numbers have continued to remain below the outbreak alert threshold and are at the average number seen at this time of the year.
For national leptospirosis hospital admissions so far this year, there have been 681 people admitted in total- noting that this includes suspected and lab-confirmed cases. Total leptospirosis hospital admissions this year by division are as follows:
380 people have been admitted to the hospital for leptospirosis in the West, with 14 new admissions last week, indicating a plateau in the trend compared to the previous week.
179 people have been admitted to the hospital for leptospirosis in Central with 5 new admissions last week, a plateauing trend compared to the admissions in the previous week. There have been 4-5 admissions a week in Central over the last 4 weeks.
103 people have been admitted to the hospital for leptospirosis in the Northern Division, with 1 new admission in the last week, which is a decrease in the admission trend compared to the 8 admissions in the week before.
19 people have been admitted to the hospital in the Eastern Division, with no new admissions since the last update.
Sadly, there are 5 new leptospirosis deaths to report since the last update on April 25th, the details of the people who died are as follows:
39-year-old male from Qamea who was admitted to CWM Hospital on April 30th, and died on 03/05/22.
31-year-old male from Ba who died at home or en-route to hospital on 02/05/22
41-year-old male from Lautoka who was admitted and died at Lautoka Hospital on 19/04/22
50-year-old male from Ba who was admitted at Lautoka hospital on 20/04/22 and died on 21/04/22
16 year old from Ba who was admitted at died at Lautoka Hospital on 13/04/22
There have been a total of 41 deaths from leptospirosis this year, with 30 in the Western Division, 4 in Central, 6 in the North, and 1 in the Eastern Division.
Prevention
The leptospirosis bacteria is spread to humans through the urine of infected animals, such as cows, pigs, rats, and dogs. To reduce your individual risk, it is important to understand that exposure to animals, soil, mud, and floodwaters during work or recreational activities increases your risk of infection.
Important prevention measures include wearing full covered footwear at all times when going outdoors, avoiding wading or swimming in flooded waters, using clean fresh water to wash up after exposure to muddy waters, and keeping all food and drinks covered and away from rats. For workplaces, practice good personal hygiene at all times, cover cuts and wounds well, and use protective equipment, especially footwear when in flooded and/or muddy areas.
We are also urging all parents and guardians to prevent children from playing in the mud or swimming in flooded rivers or creeks, and ensure that they wear shoes when outside.
Symptoms and treatment
Early treatment can decrease the severity and duration of the disease. Please seek medical care if you have recently had contact with floodwaters, mud, or animals, and develop the following symptoms: fever, muscle pain, or headache. You may also have red eyes, loss of appetite, nausea/vomiting, dizziness, or feel weak.
Leptospirosis can be treated with appropriate antibiotic medications prescribed by a doctor if treatment is sought early. Danger signs for severe leptospirosis include shortness of breath, coughing blood, chest pain, yellow eyes/skin (jaundice), signs of bleeding (including unexplained bruising), decreased or increased urination, and difficulty staying awake. Severe leptospirosis is life-threatening, and anyone with these symptoms must be taken to the hospital immediately.
Typhoid fever
There have been 116 lab-confirmed cases of typhoid fever this year, with 5 new cases since the last update.. Case numbers at the national level, and in the 4 divisions, are currently at the average level expected at this time of the year for this endemic disease.
There have been no new deaths caused by typhoid fever since the last update. There have been 6 deaths confirmed to have been caused by typhoid fever this year.
Typhoid fever is typically found in areas that do not have access to proper toilet facilities and/or clean drinking water. We strongly encourage people who live in rural areas, informal urban areas, and any other areas where access to clean drinking water is limited, to boil all drinking water. We must all also continue to practice basic hygiene measures such as frequently washing hands with soap and water, especially after visiting the toilet and before eating or preparing food.
Dengue Fever
There have been 1960 lab-confirmed cases of dengue fever this year, with 92 new cases since the last update. Case numbers are below the average numbers seen at this time of the year nationally, as well as in the Central, Eastern, and Northern Divisions.
Case numbers in the Western Division are now below the outbreak alert threshold and at the expected level seen at this time of the year, though a slight upward trend has been noted in the last week. There have been 730 cases of dengue fever recorded in the Western Division this year.
We continue to urge everyone to get rid of potential mosquito breeding places, such as empty containers inside and outside your homes that may collect water, including discarded tires, flower vases, and pot plant bases. Protect yourself from being bitten by mosquitoes by using mosquito screens in your home, and mosquito repellents.
Cold and flu
The Ministry of Health and Medical Services has noted an increase in people becoming ill with cold and flu-like illnesses as we are coming into our dry and cold season. This increase is especially seen in infants and children under the age of 5. The paediatrics department at CWM Hospital is also seeing an increase in children under the age of 5, especially infants, being admitted with acute respiratory illnesses while testing negative for COVID-19 and influenza. It has been expected that as restrictions intended to prevent transmission of COVID-19 were lifted (including mandatory masking, physical distancing, and school and border closures) other respiratory viruses that normally circulate would begin to re-emerge similar to pre-COVID levels, and possibly even at higher levels due to a decrease in population immunity to seasonal viruses, as cold/flu cases were low during the last two years.
Care for children with cold and flu symptoms
Keep your child hydrated to reduce cold and flu symptoms and help them feel better. Fevers can result in dehydration. Your child may not feel as thirsty as they normally would, and they may be uncomfortable when drinking, so it is important to encourage them to drink plenty of fluids like fresh fruit juices and water (e.g. lemon juice).
Dehydration can be very serious in babies, especially if they’re under 3 months old. Go immediately to your nearest health centre or doctor if you suspect your baby is dehydrated. Some signs may include:
no tears when crying
dry lips
a soft spot in the head that seems sunken-in
decreased activity
urinating less than three to four times in 24 hours
If your child is breastfed, attempt to breastfeed them more frequently than usual. Your baby may be less interested in breastfeeding if they’re sick. You may have to have several short feeding sessions or express breast milk and give in a small cup in order for them to consume enough fluid.
Clear up stuffed nasal passages and loosen mucous to ease cough
Careful use of a steam source in a closed room can help to relieve a stuffed nose and soften mucous to make coughing up mucous easier.
Saline drops for the nose can also be bought at pharmacies to soften nasal mucous and facilitate its discharge
Alternatively use a small amount of Vicks rub mixed with oil over the heels of feet for children >3 months old
If your child is over 1-year-old, try giving honey for a cough instead of medication. You can give 2 to 5 millilitres (mL) of honey a few times during the day.
Encourage rest
Extra rest can help your child recover faster.
Fever
Your child may be very hot due to fever. Dress them lightly and avoid heavy blankets or excessive layers that could make them feel hotter. A mild fever does not need treatment as fever is the body’s way of fighting off an infection. A lukewarm bath can also help them cool off and wind down before taking a nap or going to sleep for the night.
Seek medical care
Sometimes even the best at-home care isn’t enough to help your little one make a full recovery. Seek medical care right away if your child has any of the following:
has a fever greater than 38°C for more than two days, or a fever of 40°C or higher for any amount of time
has a fever of 38°C or higher and is under 3 months old
has a fever that doesn’t get better after taking Panadol
seems unusually drowsy or lethargic
won’t eat or drink
is wheezing or is short of breath
Prevention
After your child recovers, there are steps you can take to prevent cold and flu in the future. Wash all surfaces they came into contact with before or during their sickness. Encourage your children and other family members to wash their hands regularly to keep germs at bay.
Teach your child not to share food, drinks, or utensils when they eat. This assists in avoiding the spread of germs between them and their friends. Keep your child out of daycare or school when they are ill, especially if they have a fever. Keep them away from others with flu-like symptoms and avoid crowds.
Since the last update, we have recorded 48 new cases of which 11 new cases were recorded on 10/05/2022; 18 new cases were recorded on 11/05/2022; 10 new cases were recorded on 12/05/2022 and 9 new cases in the last 24 hours ending at 8 am this morning.
Of the 48 cases recorded, 10 cases were recorded in the Central Division; 38 cases were recorded in the Western Division and nil cases were recorded in the Northern and Eastern Division.
The national 7-day rolling average of cases as of 9th May is 10 daily cases.
In the 7 days until 12/05/2022, 14 new cases were recorded in the Central division, 56 new cases in the Western division and nil new cases in the Northern and Eastern Divisions.
The Central Division cases constitute 67% of the cumulative total cases nationally, with the Western division making up 28%, 3% in the Northern Division, and 2% in the Eastern Division.
Deaths:The curve depicts daily COVID-19 deaths by division since May 2021. It indicates a surge from last December, with peaks in mid-January 2022 followed by a downward trend, with the most recent death occurring on March 4th 2022.
There is no COVID-19 death to report today.
Analysis of Deaths in the Third Wave
Table 1: Death rates by Division
Division
Total COVID Deaths
Deaths per 100,000
Central
61
15.4
Western
67
18.8
Northern
28
20.0
Eastern
5
13.0
An analysis of the 161 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population.
Table 2: Deaths by Age Group
Age Group
Total Deaths
Deaths per 100,000
population
0 – 9
6
3.3
10-19
2
1.3
20-29
3
2.1
30-39
4
2.9
40-49
6
5.4
50-59
21
23.1
60-69
33
63.5
70-79
50
223.2
80-89
28
497.6
90-99
6
1153.8
For the 161 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition.
Table 3: Deaths by Vaccination Status
Age Cohort
Total COVID deaths
Total Vaccinated/ Unvaccinated
Deaths per 100,000 Vaccinated Population
Deaths per 100,000 Unvaccinated Population
>18
129
59/94
10.1
275.2
15-17
1
0/1
0
6.6
12-14
1
0/1
0
2.5
Out of 161 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 161 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.1 per 100,000 population for fully vaccinated adults and 275.2 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 27.2times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine.
There have been a total of 862 deaths due to COVID-19 in Fiji. As of April 24th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported.
We have also recorded 939 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths.
Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, there are nil cases in the asymptomatic, mild, moderate, severe and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community.
Testing:
635 tests have been reported for May 12th, 2022. Total cumulative tests since 2020 are 517,703 tests. The 7-day daily test average is 706 tests per day or 0.8 tests per 1,000 population.
The national 7-day average daily test positivity is 1.3%, which is within the WHO recommendation of 5%.
Public Advisory
Engaging COVID safety without mandates or quarantine
Since the 7th of April and the lifting of our quarantine measures and increased international travel, our community and border surveillance screening data continue to report a low positivity rate despite the ongoing pandemic, and the continued evolution of Omicron variants. While there is a low positivity rate among arrivals we are seeing positive arrivals. We are also aware that a key aspect of living with Covid is to have a strong community surveillance system within the community AND at the border. This will allow early identification of community outbreaks and facilitate early response. Early response capability is a key part of mitigating the risk of severe disease and severe containment measures and to further easing pre-departure conditions for international travel. As part of our community surveillance exercise, we will be transitioning to t9he more routine use of throat and nasal swabs as opposed to the more uncomfortable nasopharyngeal swabs
The Ministry informs the public that for the positive cases among arrivals, existing protocols have been instituted to ensure travellers that return positive COVID-19 test results follow protocols and isolate for the required 7 – days as advised.
However, the Ministry is concerned that there are travellers who are not adhering to the 7-days of isolation and continue to be mobile during that 7-day isolation period.
We call on the public to support the protection and safety of all Fijians by reminding travellers from overseas who are visiting friends and relatives of the importance of isolating themselves for 7 days if they test positive for COVID-19. As a nation, Fiji has emerged from the period of restrictions that were instituted to protect our people and our country from COVID-19. We need not be reminded of the high number of positive cases and the number of deaths from COVID-19. The Ministry reiterates that the lifting of masking and other mandates and easing of travel restrictions is NOT a sign that the risk of outbreak and resurgence of COVID-19 is over. It is important that we continue to work together to protect ourselves, our communities and our country from any further
The following prevention measures continue; the promotion of vaccination, personal COVID-safe hygiene habits, and workplace ventilation and air cleaning measures. We recommend everyone continue to employ COVID-safe measures to prevent infection and the spread of infection: Frequently wash your hands or use an alcohol-based hand sanitiser, stay home if you feel sick, cover your mouth and nose with a tissue or the bend of your elbow if you cough or sneeze, wear a mask if you have any signs of a respiratory illness.
We have dropped the pre-departure testing requirement for travellers coming into Fiji and also we now require international arrivals to test within 72 hours of arrival. Beyond this potential change, our border protection will be mediated by the fact that all travellers over 16 years are vaccinated. Inbound travellers aged 12 years and above must produce proof of a pre-booked and pre-paid rapid antigen test, to be administered within 72 hours of arrival in Fiji. Booking for tests can be made through this link: https://entrytestfiji.com. There will be exemptions for those who have tested positive and recovered from COVID-19 within the 30 days before travel and have fit-to-fly certificates. Failure to comply with arrival testing once in Fiji will result in a spot fine of $1000.
Ongoing Medical Recovery Efforts
With the reduction in COVID-19 cases and in people presenting to health centres with acute respiratory illness, the MOHMS team is in a better position to focus more on health facilities and health care provision capabilities so as to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment.
Our command centres and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and to work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
We are also focused on carrying out general health service work more efficiently in all facilities, and a key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is a strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities and allow for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision making and action within the Ministry.
COVID-19 Vaccination
As of the 13th of May, a total of 126,726 (29.5%) individuals have so far received booster doses. This represents 29.3% of those eligible for a booster dose. The booster dose interval for eligible persons has been reduced to 3 months from the 2nd dose. This is in recognition of the risk of disease surge based on waning 2 doses covid vaccine protection, slow booster uptake, increased international travel with the relaxation of border measures, and ongoing outbreaks in various parts of the world. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The public is urged to get booster vaccine doses, and the list of vaccination sites is provided daily on the MOH. We have accepted an offer of 50,000 doses of Pfizer paediatric doses for children aged 5 to 11 by the Aotearoa New Zealand Government. Our vaccination team is currently discussing with counterparts in NZ on further details while our efforts to source more through our other development partners are ongoing.
Our school vaccination program has also been progressing such that with the 95% adult coverage rate, 90.6% of all persons over 12 years have had 2 doses of the COVID-19 vaccine.
We will continue to monitor the evidence on post-infection immunity based on quality data generated globally. However, until we have a better sense of the role of post-infection immunity, the Ministry of Health will continue to define our level of protection based on vaccination numbers
Given the current stocks of Pfizer vaccines, we are now covering the Primary doses for those yet to be vaccinated and for Dose 2 if individuals were vaccinated with either Moderna or Astra Zeneca while the 12-14-year-olds continue with the Pfizer vaccine. The new supplies of MODERNA are expected to be available in-country at the end of the month.
Multi-country acute hepatitis of unknown origin
The Ministry of Health and Medical Services has been monitoring reports of acute hepatitis (liver inflammation) of unknown origin in children in multiple countries including the United Kingdom, the United States of America, Spain, Israel and France. According to the World Health Organisation, there have been 169 cases as of April 21st in 11 countries. We understand that studies into the cause of this illness in children are ongoing, and we continue to monitor reports by the World Health Organisation and other country health authorities as the investigation progresses. We have alerted our specialist children’s doctors within the Ministry, and to date, we have had no reports of cases in Fiji.