COVID-19 Update
Wednesday 20th April

| Transmission Update:
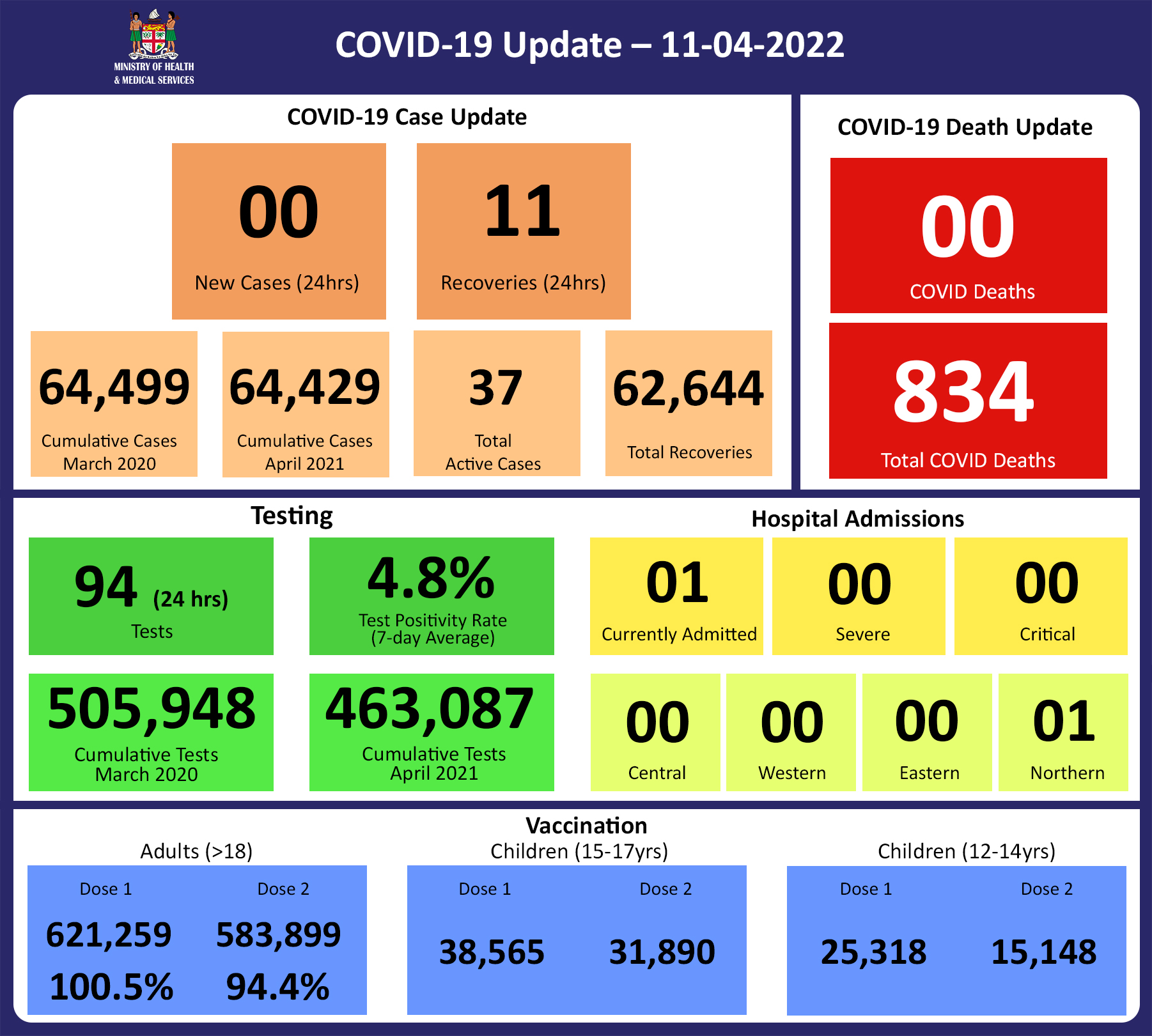
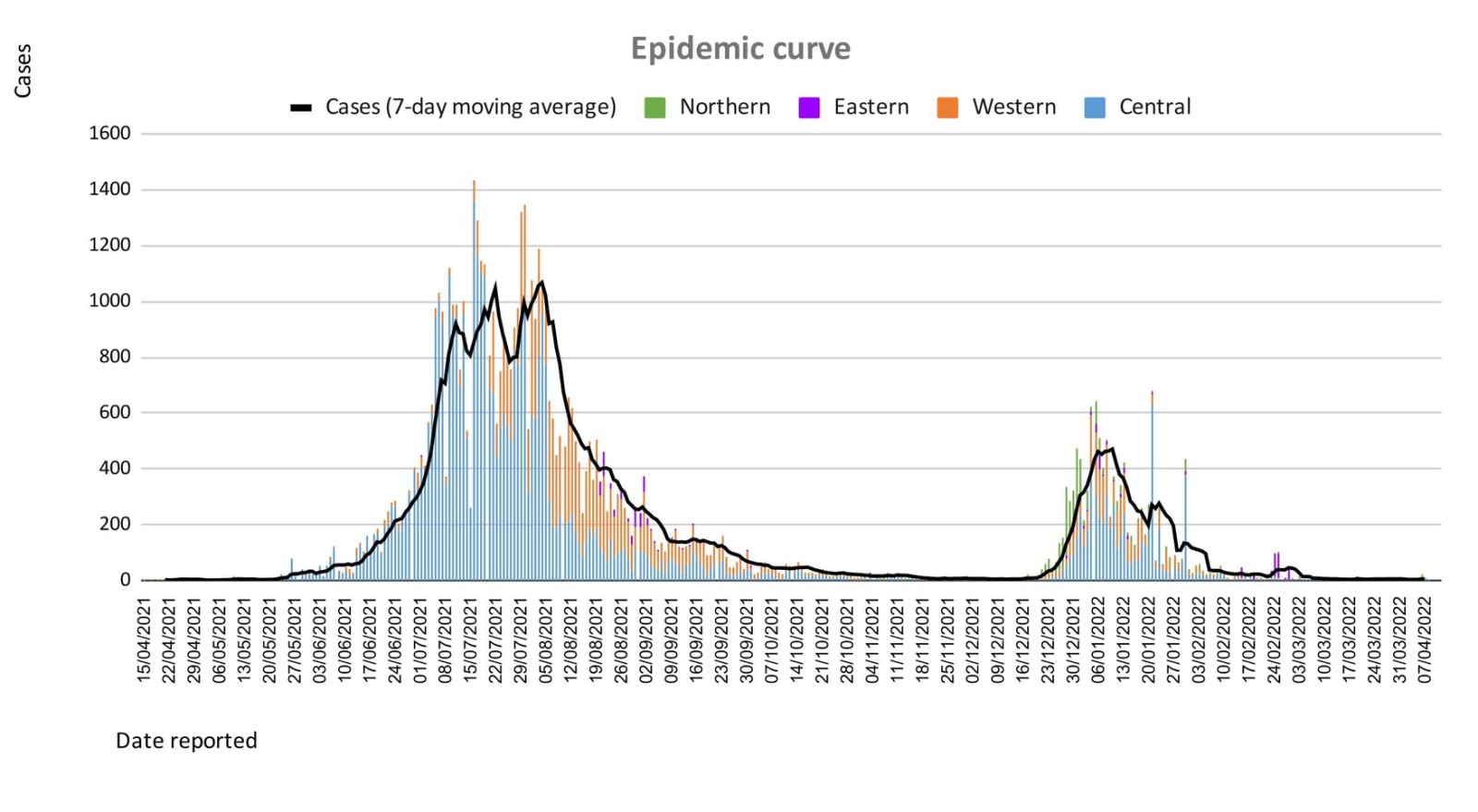
Since the last update, we have recorded 11 new cases of which 9 new cases were recorded on 19/04/2022 and 2 new cases in the last 24 hours ending at 8 am this morning. Of the 11 cases recorded, 2 cases were recorded in the Central Division; 9 cases were recorded in the Western Division and nil cases were recorded in the Northern and Eastern Division. The national 7-day rolling average of cases as of 16th April is 2 daily cases. In the 7 days until 19/04/2022, 1 new case was recorded in the Central division, 17 new cases in the Western division, 1 new case in the Northern Division, and nil new cases in the Eastern Division. The Central Division cases constitute 68% of the cumulative total cases nationally, with the Western division making up 27%, 3% in the Northern Division, and 2% in the Eastern Division. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
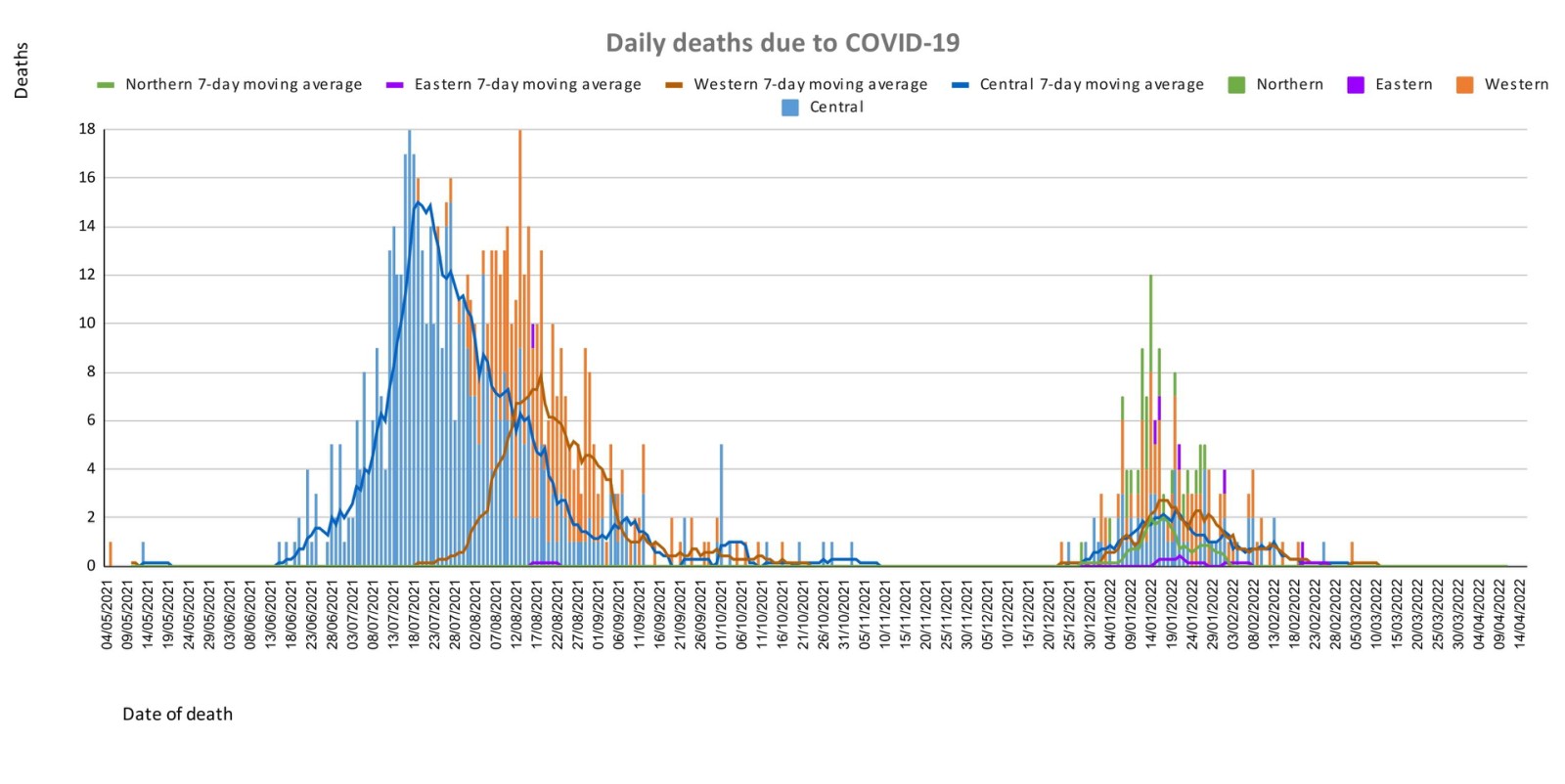
| Deaths:
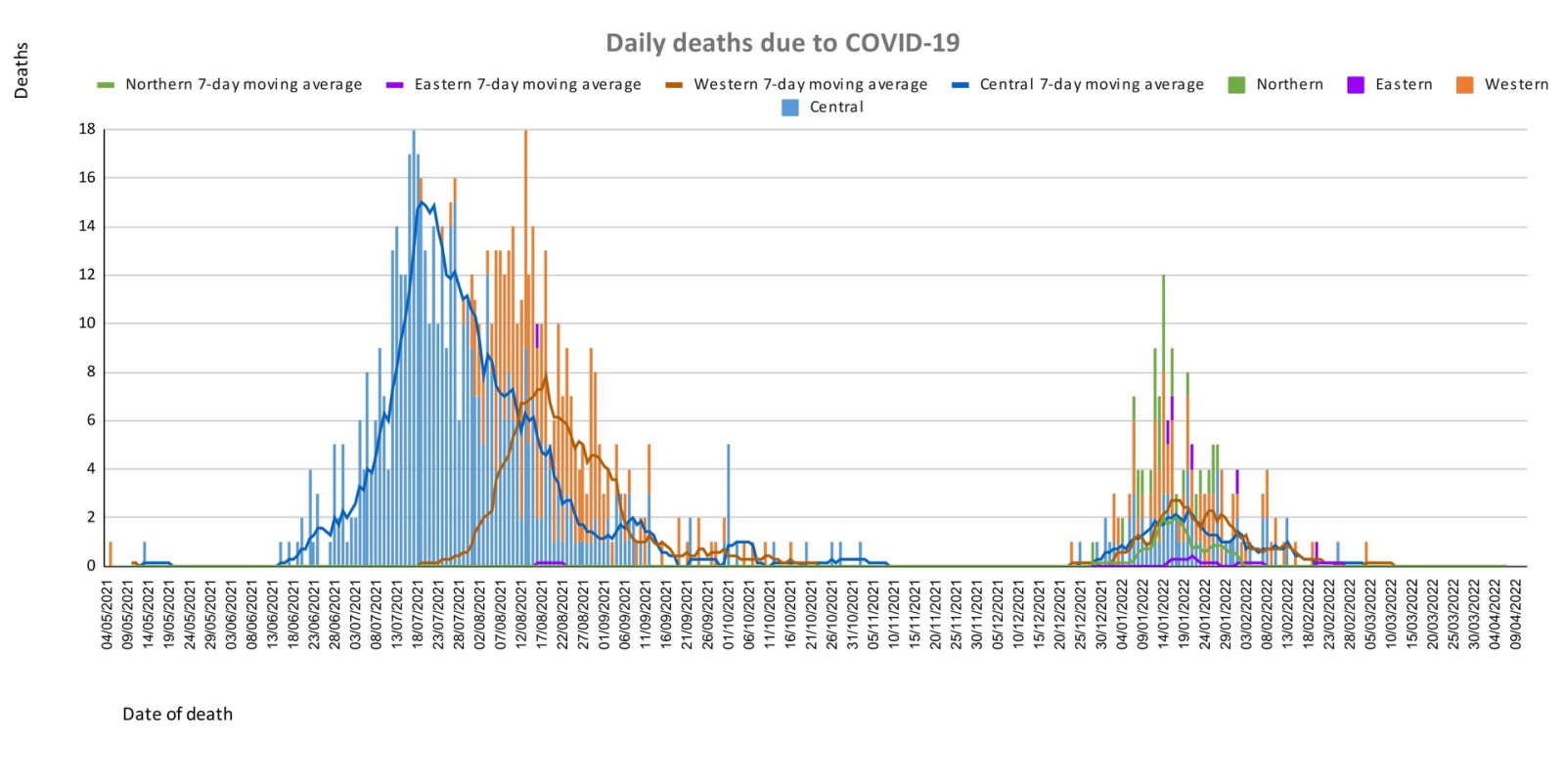
The curve depicts daily COVID-19 deaths by division since May 2021. It indicates a surge from last December, which peaks by mid-January 2022 followed by a downward trend, with the most recent death occurring on March 4th. (Note: in the last two weeks, a COVID death audit was carried out by the MOHMS and an additional 28 unreported COVID deaths were obtained from western health facilities, this explains the sudden change in graph patterns and reporting numbers- details of the audit are explained below). New Deaths to Report There is no new COVID-19 death to report today. Analysis of Deaths in the Third Wave Table 1: Death rates by Division
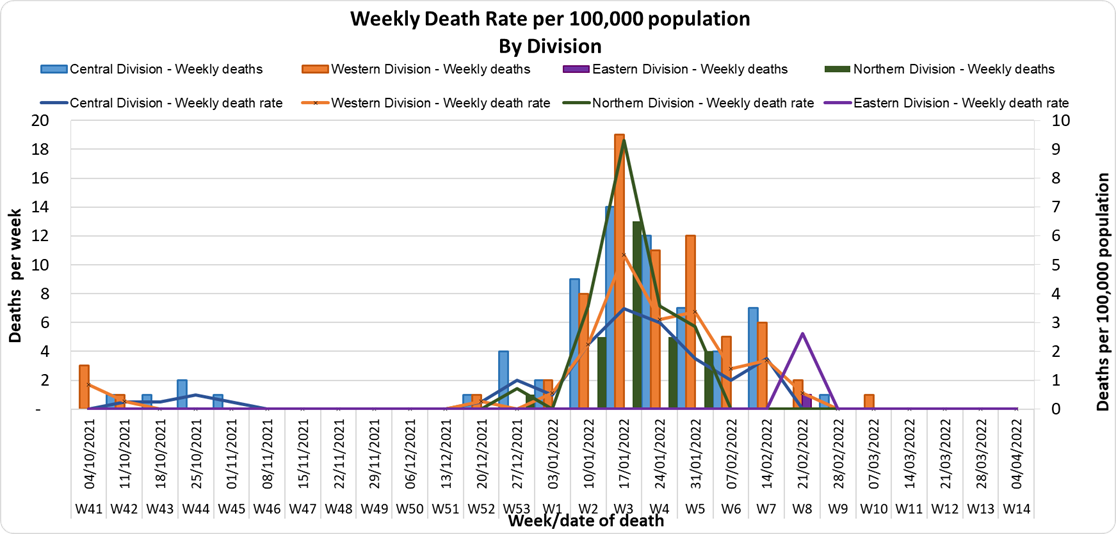
An analysis of the 161 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population. Table 2: Deaths by Age Group
For the 161 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition. Table 3: Deaths by Vaccination Status
Out of 161 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 161 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.1 per 100,000 population for fully vaccinated adults and 275.2 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 27.2 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine. There have been a total of 862 deaths due to COVID-19 in Fiji. As of April 16th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported. We have also recorded 939 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, 50% (n=1) are categorised as asymptomatic and mild; 50% (n=1) are categorised as moderate, will nil cases in the severe and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community. The number of people being admitted because of COVID-19 remains low. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Testing:
220 tests have been reported for April 19th, 2022. Total cumulative tests since 2020 are 506,642 tests. The 7-day daily test average is 79 tests per day or 0.1 tests per 1,000 population. The national 7-day average daily test positivity is 5.6%, which is above the WHO recommendation of 5%. |


Public Advisory
Engaging COVID safety without mandates or quarantine
Since the 7th of April and the lifting of our quarantine measures and increased international travel, our community and border surveillance screening data continue to report a low positivity rate despite the ongoing pandemic, and the continued evolution of Omicron variants.
The lifting of masking and other mandates, and easing of travel restrictions, is NOT a sign that the risk of outbreak and resurgence of COVID-19 is over. We reiterate the need for each individual to assess their own level of risk and decide to continue to take measures such as masking and physical distancing. For example, we know that wearing a mask in public will lower your risk of getting infected, and it is now an individual choice and responsibility that is recommended by the Ministry. If you are at higher risk of severe disease should you get infected with COVID-19, we strongly recommend that you continue to wear a mask in public, particularly in crowded indoor spaces. The promotion of COVID-safe measures will now be pursued similar to how we advise healthy lifestyle measures for the prevention of non-communicable diseases, and how basic hygiene is promoted for the prevention of infectious diseases like typhoid fever. The measures that will continue in terms of prevention are the promotion of vaccination, personal COVID-safe hygiene habits, and workplace ventilation and air cleaning measures. We recommend everyone continue to employ COVID-safe measures to prevent infection and the spread of infection: Frequently wash your hands or use an alcohol-based hand sanitiser, stay home if you feel sick, cover your mouth and nose with a tissue or the bend of your elbow if you cough or sneeze, wear a mask if you have any signs of a respiratory illness.
We also note the risk of transmission in children under 12 years, and as such we are exploring the option of requiring children under the age of 12 to also undergo pre-departure testing before travelling to Fiji. Beyond this potential change, our border protection will be mediated by the fact that travellers are vaccinated, have a negative pre-departure test, and will be tested in-country with a rapid antigen test. Currently, inbound travellers aged 12 years and above must produce proof of a pre-booked and pre-paid rapid antigen test, to be administered after 48 hours, but before 72 hours of arrival in Fiji. Booking for tests can be made through this link: https://entrytestfiji.com. There will be exemptions for those who have tested positive and recovered from COVID-19 within the 30 days before travel and have fit-to-fly certificates. Failure to comply with arrival testing once in Fiji will result in a spot fine of $1000.
Ongoing Medical Recovery Efforts
With the reduction in COVID-19 cases and in people presenting to health centres with acute respiratory illness, the MOHMS team is in a better position to focus more on health facilities and health care provision capabilities so as to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment. Our command centres and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and to work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
A key focus is also on carrying out general health service work more efficiently in all facilities. With the return from annual leave of our much needed corporate staff, the process of reporting and prioritising general works, and ensuring they are communicated clearly and tracked through our command centre and operation will be improved. A key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is also seen as a key strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities. The framework will allow greater ability for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision making and action within the Ministry.
COVID-19 Vaccination
As of the 20th of April, a total of 121,714 individuals have so far received booster doses. The booster dose interval for eligible persons has been reduced to 3 months from the 2nd dose. This is in recognition of the risk of disease surge based on waning 2 doses covid vaccine protection, slow booster uptake, increased international travel with the relaxation of border measures, and ongoing outbreaks in various parts of the world. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The public is urged to get booster vaccine doses, and the list of vaccination sites is provided daily on the MOH webpage. Given the competing health priority issues, I have instructed our health teams to go back to the health facilities and do targeted booster programs for the vulnerable and the willing and to focus on our 12 to 18-year-olds through the school vaccination program. Furthermore, we can confirm that we have accepted an offer of 50,000 doses of Pfizer paediatric doses for children aged 5 to 11 by the Aotearoa New Zealand Government. Our vaccination team is currently discussing with counterparts in NZ on further details while our efforts to source more through our other development partners are ongoing.
Our school vaccination program has also been progressing such that with the 94% adult coverage rate, 88% of all persons over 12 years have had 2 doses of the COVID 19 vaccine.
We will continue to monitor the evidence on post-infection immunity based on quality data that is being generated globally. However, until we have a better sense of the role of post-infection immunity, the Ministry of Health will continue to define our level of protection based on vaccination numbers
Given the current stocks of Pfizer vaccine we have we are using the Pfizer vaccine for the ongoing primary 2 dose schedule of children and adults, and as the booster dose.
Our statements will be released on Monday and Thursday starting next week. Hence the next statement following this will be on Monday 25th April.