COVID-19 Situation Update
Monday 28th February
| Transmission Update:
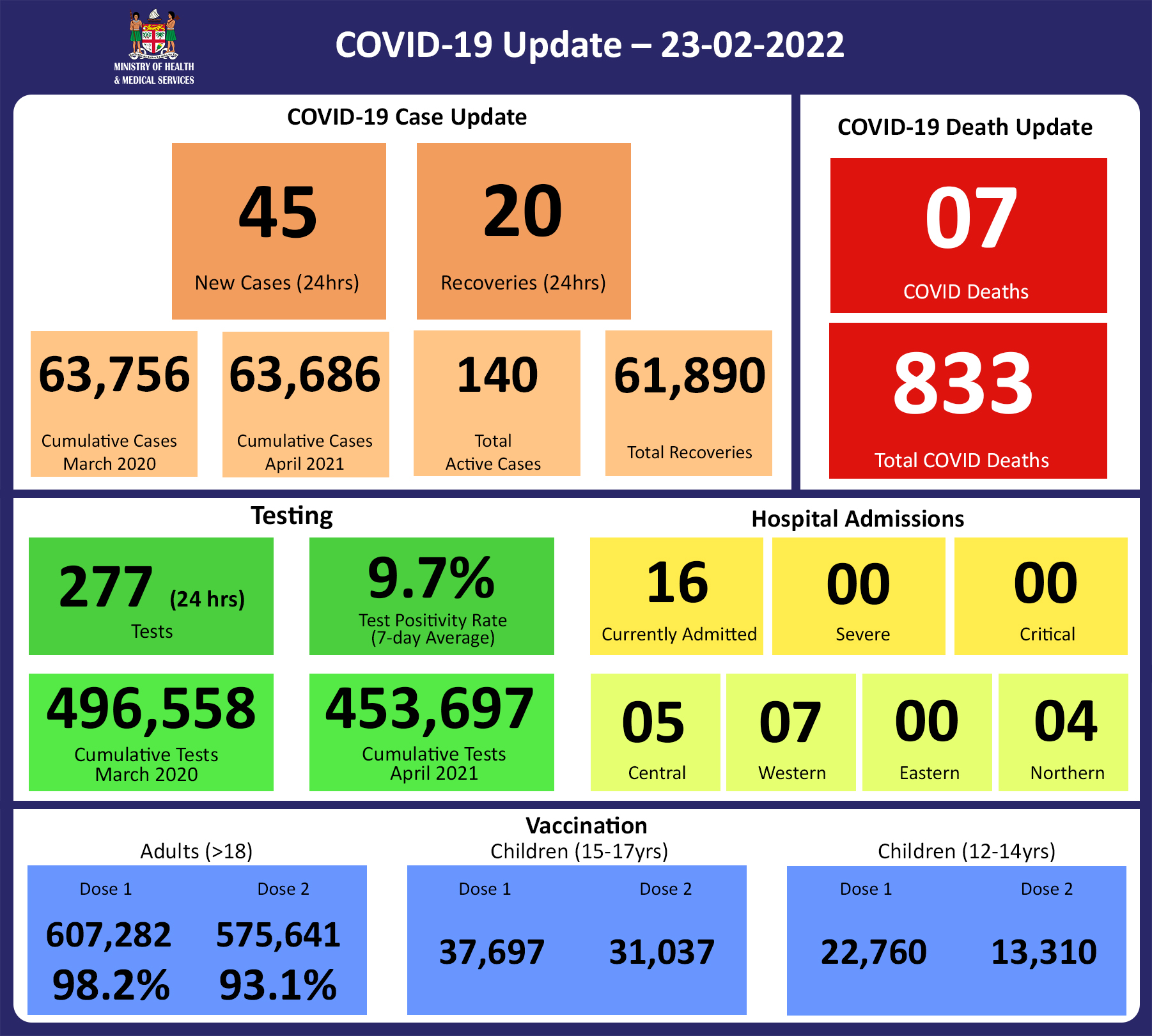
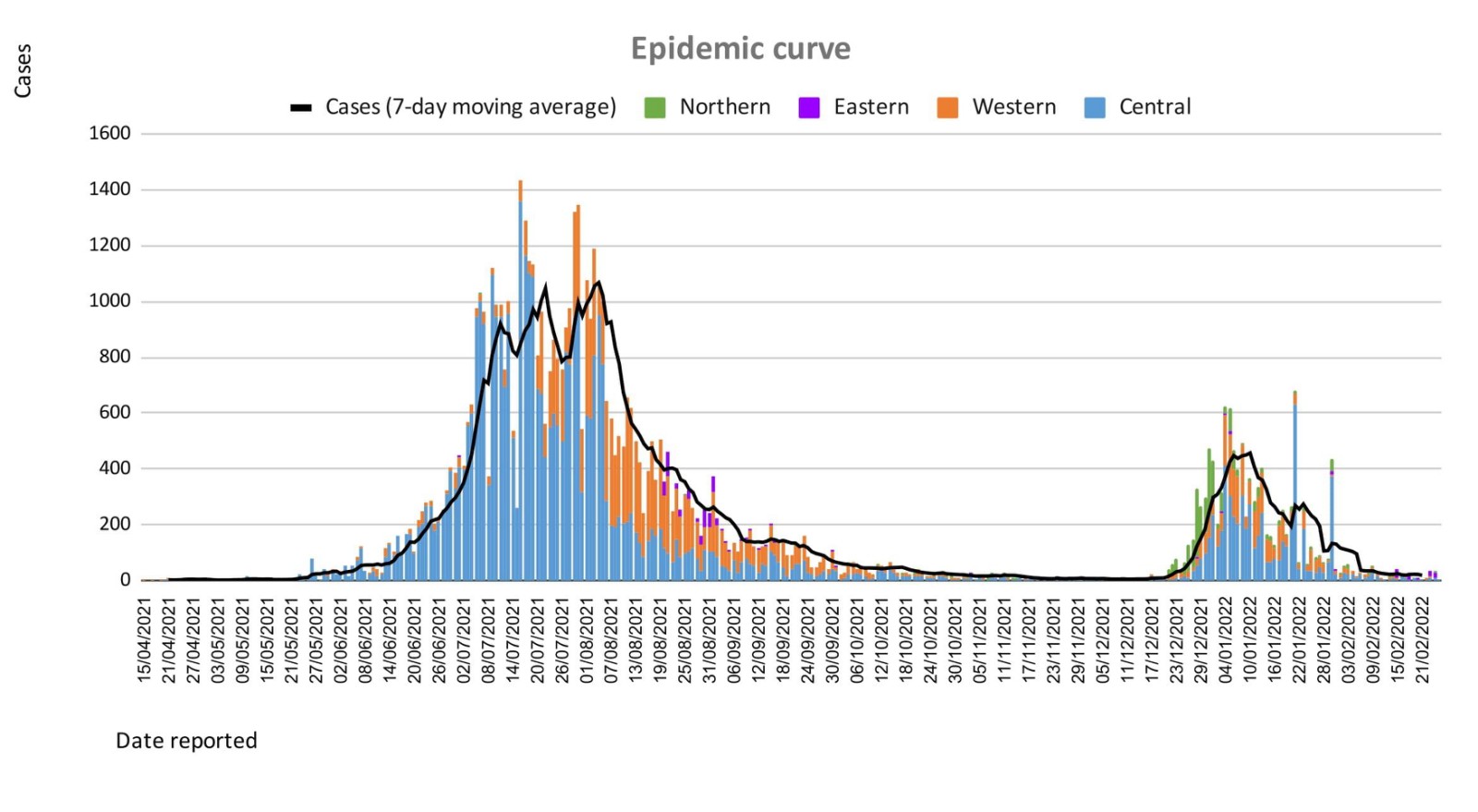
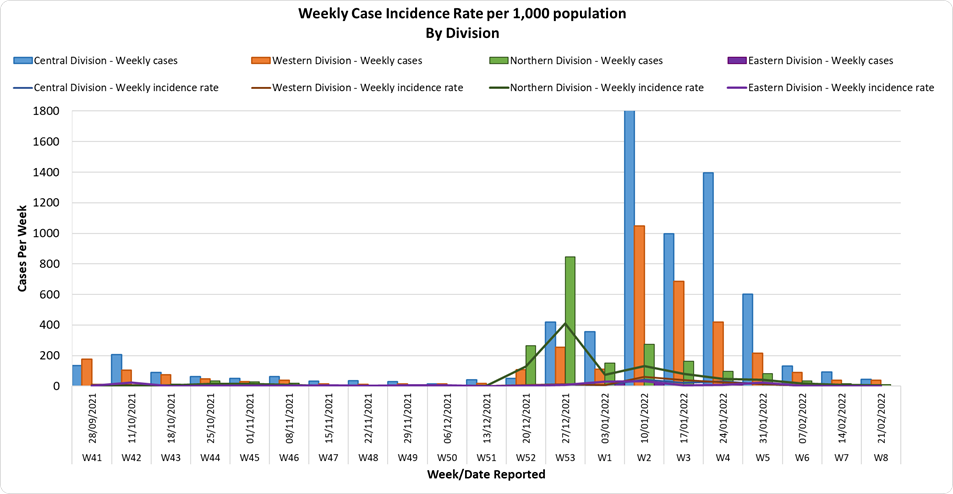
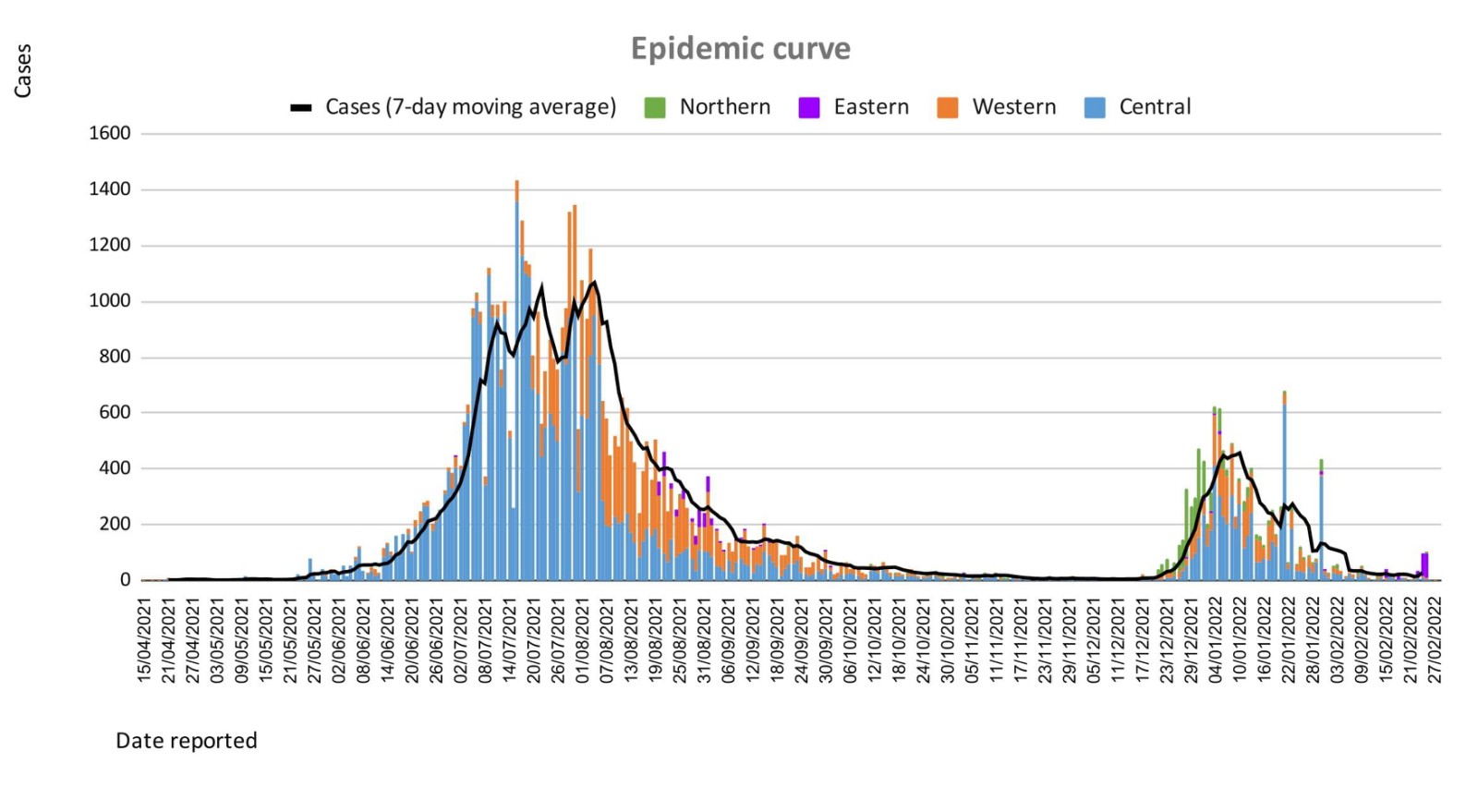
Since the last update, we have recorded 103 new cases of which 97 new cases were recorded on 26/02/2022; 4 new cases were recorded on 27/02/2022 and 2 new cases in the last 24 hours ending at 8 am this morning. Of the 103 cases recorded, 8 cases were recorded in the Central Division; 7 cases were recorded in the Western Division, 4 cases were recorded in the Northern Division, and 84 cases were recorded in the Eastern Division. Overall, there have been 63,860 cases of COVID-19 recorded in Fiji, with 68% of the cases from the Central Division, 28% of the cases from the Western Division, 1% of the cases from the Eastern Division, and 3% from the Northern Division. The national 7-day rolling average of cases as of 24th February is 28 daily cases. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Deaths:
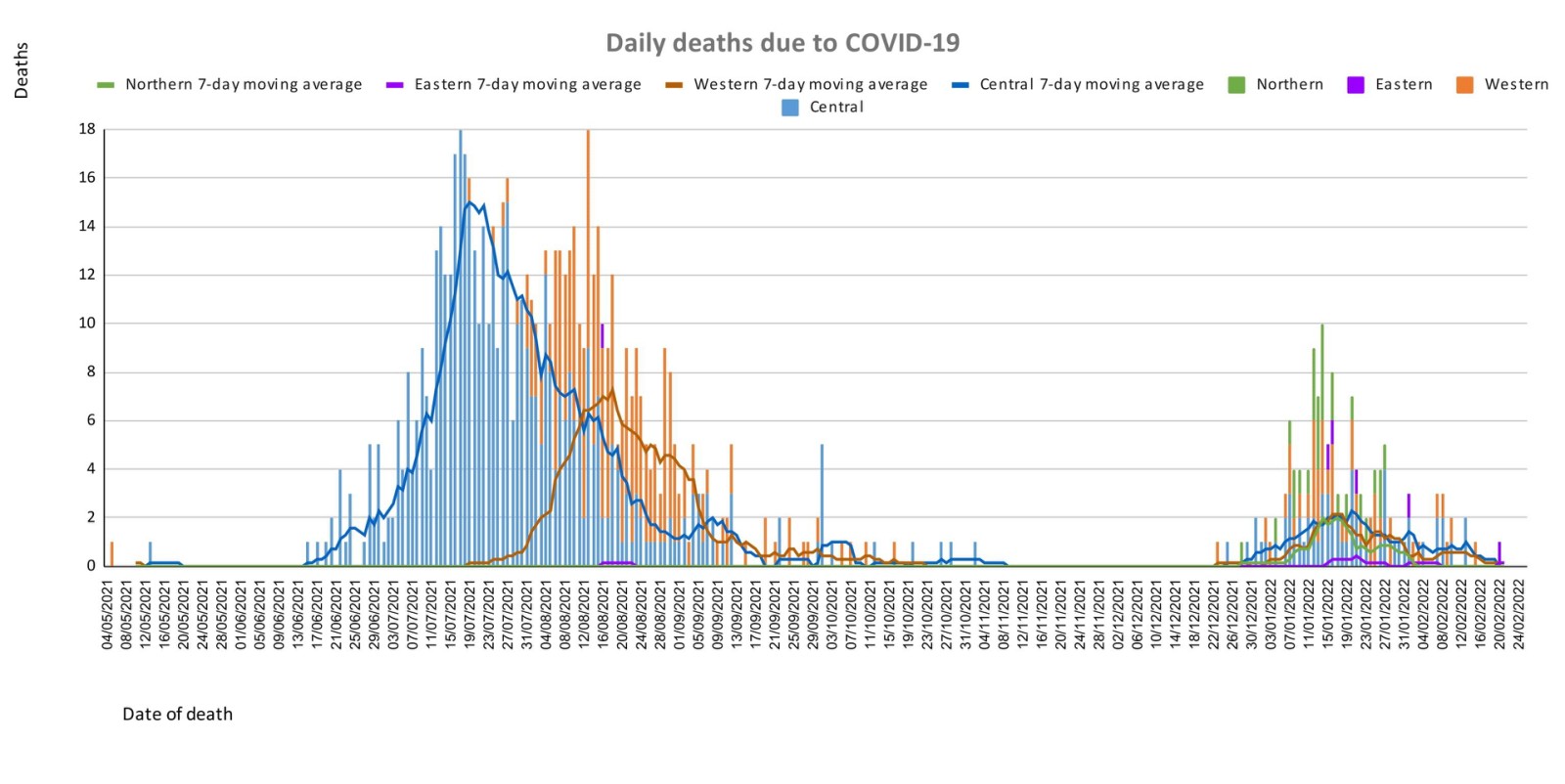
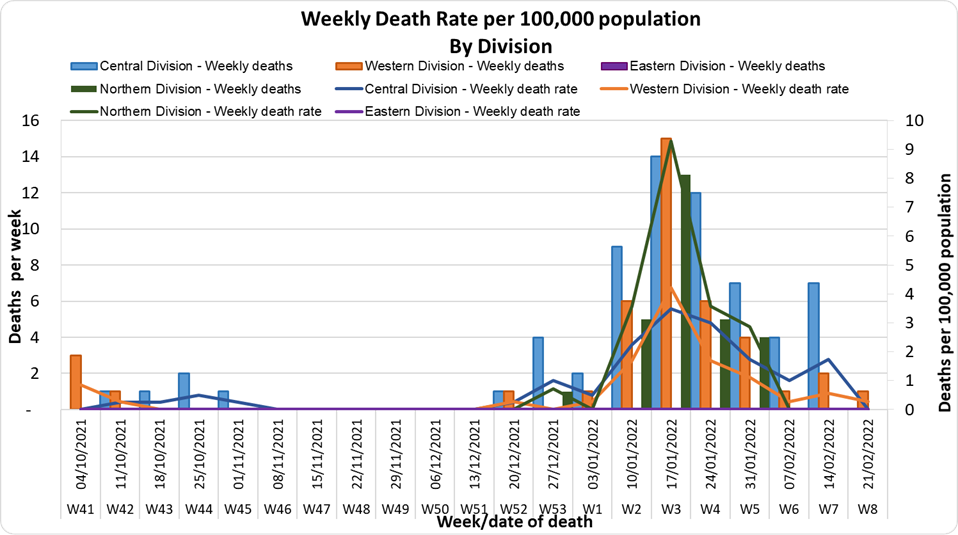
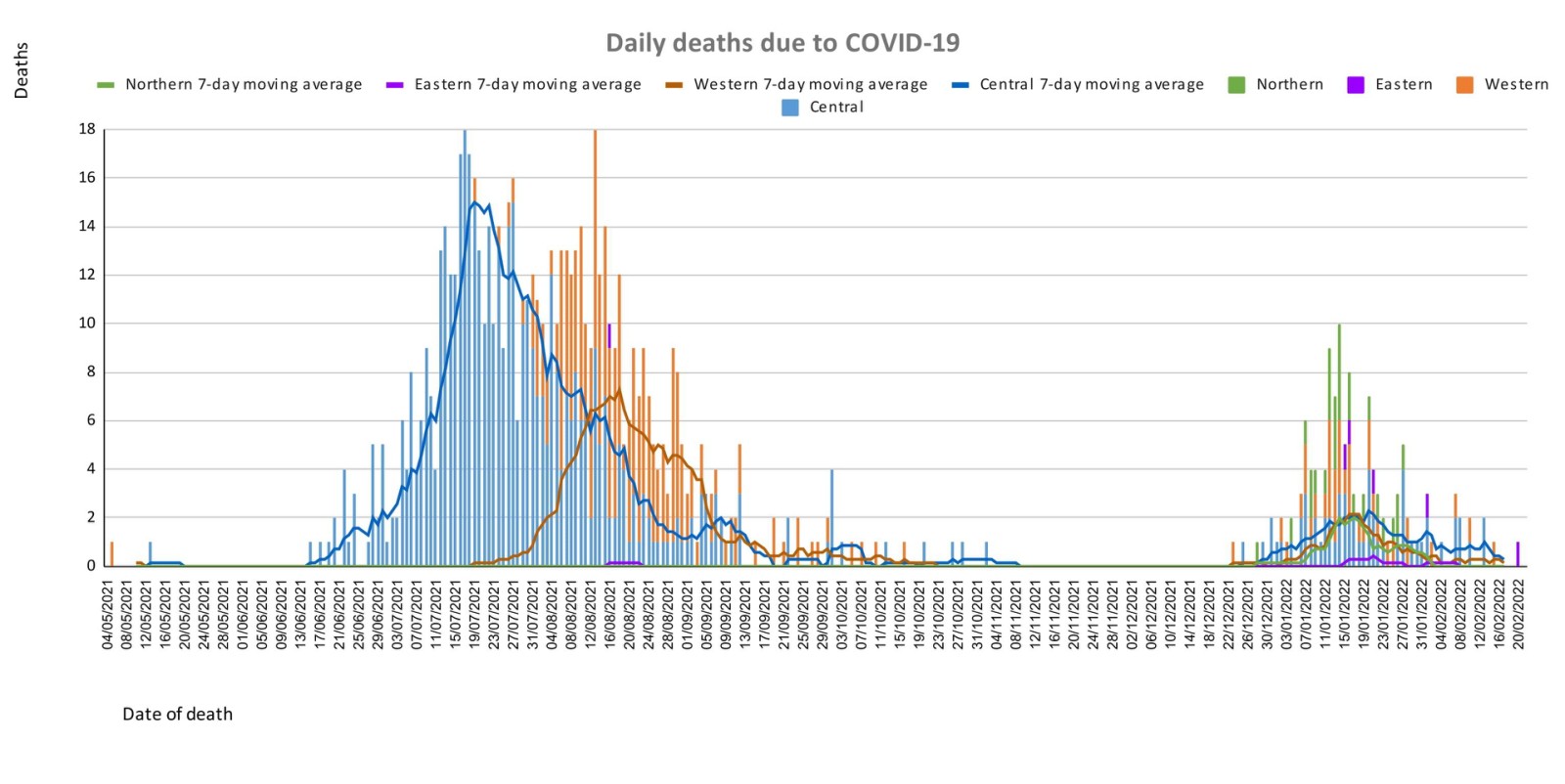
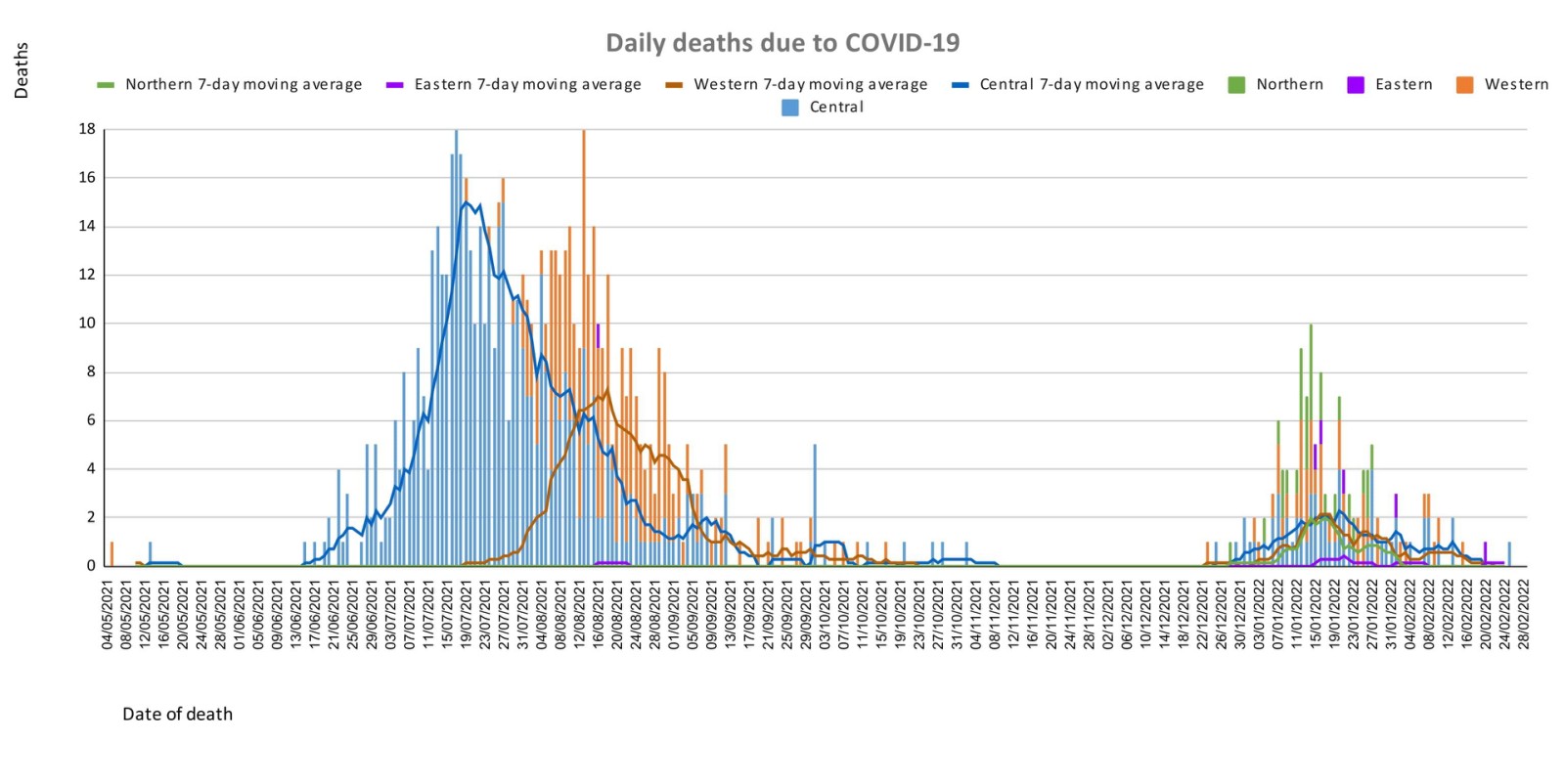
The curves depict weekly COVID-19 deaths by division since May 2021. It indicates a surge from December-end 2021, which peaks by mid-January 2022. The 3rd COVID 19 wave is considered to have started around mid to late December 2021. (Note: Death notifications from within the last two weeks are still being received, therefore the graphs may alter slightly upon reporting). Analysis of Deaths in the Third Wave Table 1: Death rates by Division
An analysis of the 138 deaths recorded in the third wave show that, while the Central Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population.
Table 2: Deaths by Age Group
Table 3: Deaths by Vaccination Status
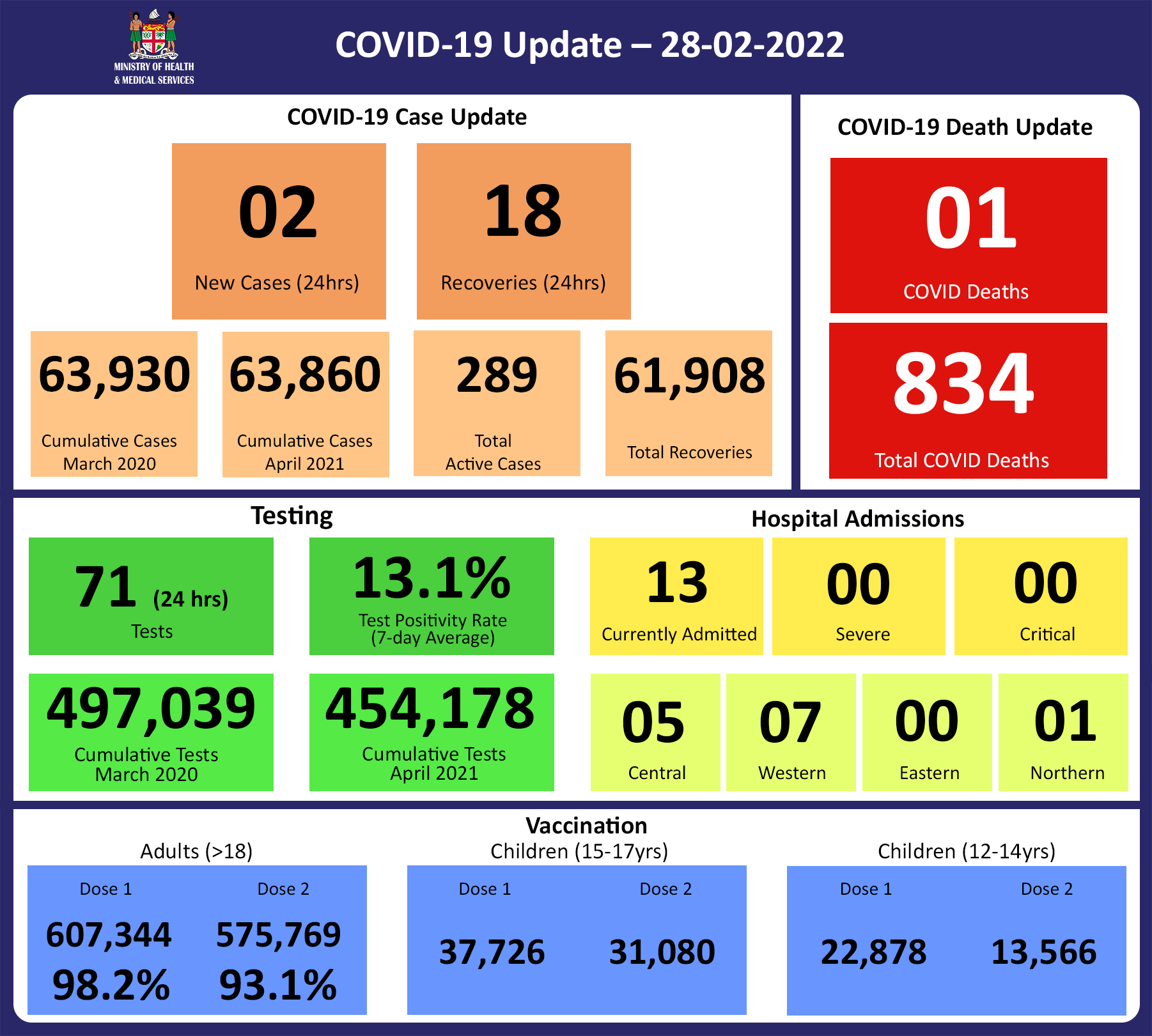
Out of 138 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 132 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, a death rate of 9.5 per 100,000 population for fully vaccinated adults and 176.3 for unvaccinated adults was exhibited. This means that unvaccinated adults in Fiji have been dying at a rate 18.5 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals of the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine. New deaths to report There is one new COVID-19 death to report. The COVID-19 death is of an 87-year-old female from the Central Division, who died at home on 25/02/2022. She was not vaccinated. There have been a total of 834 deaths due to COVID-19 in Fiji. Please note that due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported. Therefore, as of February 24th, 2022, the national 7 days rolling average for COVID-19 deaths per day is 0.1, with a case fatality rate of 1.29%. We have recorded 897 COVID-19 positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hospitalization:
There is a sustained downward trend in daily hospitalizations. Using the WHO clinical severity classification, a greater percentage, 61% (n=8) of the admissions of COVID-19 positive patients are categorised as asymptomatic and mild, 31% (n=4) is categorised as moderate and 8% (n=1) as severe with nil cases in the critical category. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community. The number of people being admitted because of COVID-19 remains low. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Testing:
71 tests have been reported for February 27th, 2022. Total cumulative tests since 2020 are 497,039 tests. The 7-day daily test average is 180 tests per day or 0.2 tests per 1,000 population. The national 7-day average daily test positivity is 13.1%. The high positivity rate is an indication of widespread community transmission. |
Public Advisory:
Leptospirosis, typhoid fever, and dengue fever
The next update on the leptospirosis outbreak will be published in the statement on Wednesday. However, reports are indicating increasing hospital admissions for cases of severe leptospirosis in the Western Division, and also now in the Central Division. Cases remain predominantly in the 10-39-year-old age group, with more cases in males than females, and a majority of cases in people of the i-Taukei ethnicity.
As mentioned in the previous updates, the new area of concern is the Ra Medical area where we have noted a marked increase in cases and hospitalisations. We have increased support to the Ra Subdivision Medical Team by mobilising a FEMAT team to man Rakiraki Hospital while the Ra Medical subdivision team will conduct outreach services to villages and communities in the Ra province. Suspected cases will be counselled on ongoing care and the severely ill will be transferred to the hospital to receive the appropriate treatment. The community outreach teams will also review chronic medical cases and update their management. Environmental Health Officers (EHOs)have also been brought in to work with the communities in escalating cleanup efforts that will help to control the population of communicable disease vectors such as mosquitoes, rats, and other rodents in affected areas. EHOs also assist to educate the communities on the risk of exposure to floodwaters and to discourage our people from playing in flooded areas and muddy places that increase their risk of contracting leptospirosis and other water-borne diseases.
Recent floods have affected many areas and communities throughout the country. The Ministry is focussing on geographical areas of concern for the purpose of mobilizing extra capability to help manage communicable disease outbreaks and also escalate the promotion of preventative measures.
To reduce your individual risk, it is important to understand that exposure to animals, soil, mud, and floodwaters during work or recreation activities increases your risk of infection.
Important prevention measures include wearing full covered footwear at all times when going outdoors, avoiding wading or swimming in flooded waters, using clean fresh water to wash up after exposure to muddy waters, and keeping all food and drinks covered and away from rats. For workplaces, practise good personal hygiene at all times, cover cuts and wounds well, and use protective equipment, especially footwear when in flooded and/or muddy areas.
Early treatment can decrease the severity and duration of the disease. Please seek medical care if you have recently had contact with floodwaters, mud, or animals, and develop the following symptoms: fever, muscle pain, headache. You may also have red eyes, loss of appetite, nausea/vomiting, dizziness, or feel weak.
Leptospirosis can be treated with appropriate antibiotic medications prescribed by a doctor if treatment is sought early. Danger signs for severe leptospirosis include shortness of breath, coughing blood, chest pain, yellow eyes/skin (jaundice), signs of bleeding (including unexplained bruising), decreased or increased urination, difficulty staying awake. Severe leptospirosis is life-threatening, and anyone with these symptoms must be taken to the hospital immediately.
The Ministry has so far recorded a lower number of cases of Typhoid fever than anticipated for the current period as in previous years. Typhoid fever is typically found in areas that do not have access to clean drinking water. We strongly encourage people who live in rural areas, informal urban areas, and any other areas where access to clean drinking water is limited, to boil all drinking water. We must all also continue to practise basic hygiene measures such as frequently washing hands with soap and water, especially after visiting the toilet and before eating or preparing food.
Recent increases in reported cases of Dengue fever from around the country remain a serious concern. We continue to urge everyone to get rid of potential mosquito breeding places, such as empty containers outside your homes that may collect water, including discarded tires. Protect yourself from mosquitoes by using mosquito screens in your homes, and mosquito repellants.
Vaccination
As of the 27th of February, a total of 103,101 individuals have so far received booster doses. Members of the public are advised to obtain their booster dose after at least 5 months from their second COVID-19 vaccine dose. Moderna vaccine and Pfizer vaccines are both available for adult booster doses.
The Ministry of Health and Medical Services will continue to monitor the advisories on post-infection immunity based on quality data that is being generated globally
Supporting International Travel
- Plan to remove 3-day hotel stay for fully vaccinated travelers from Travel Partner Countries.
Since the opening of international travel borders to travel partner countries travelers coming in from Travel Partner Countries have had to undergo an in-country test in Fiji on day 2 of stay in Fiji. To support this requirement, a 3-day hotel stay was mandated to minimize the risk of non-compliance to testing and to ensure that all positive tests were appropriately responded to while the traveller was locatable. To be clear, this 3-day stay in a Care Fiji Commitment (CFC) hotel was never a quarantine. The hotel stay is in place to facilitate the testing requirement on day 2 of arrival.
We have noted that while many countries have removed all forms of traveller sequestration, the in-country testing conditions continue. As such we are supporting current efforts to have more testing sites throughout Fiji to which travellers can book for testing, without requiring a hotel stay, as part of prior approval to come into Fiji. We are working together with the Ministry of Trade and Tourism and Ministry of Economy in the final phase of approving this in-country testing for international arrivals by private entities. These private entities will ensure that the test is available and the results will be reported back to Ministry of Health officials. They will also be mandated to report any international traveller who defaults from the mandatory testing. Any traveller defaulting a test will be subject to legal punitive measures.
- Ongoing Review of Non-Travel Partner Country Status
This ongoing effort is mediated through the Ministry of Commerce, Trade, Tourism and Transport, and the Ministry of Economy (COVID-19 Risk Mitigation Taskforce). Non-Travel Partner Status is assessed and graduated to Travel Partner status based on COVID-19 Transmission Data (cases, admission, and deaths), COVID-19 Community Surveillance data (Test per 1000, positivity rate), and ability to detect Variants (Access to genomic sequence capability). A list of Travel partner countries is available on the following link.