
COVID-19 Update
Thursday 30th June
| Transmission Update:
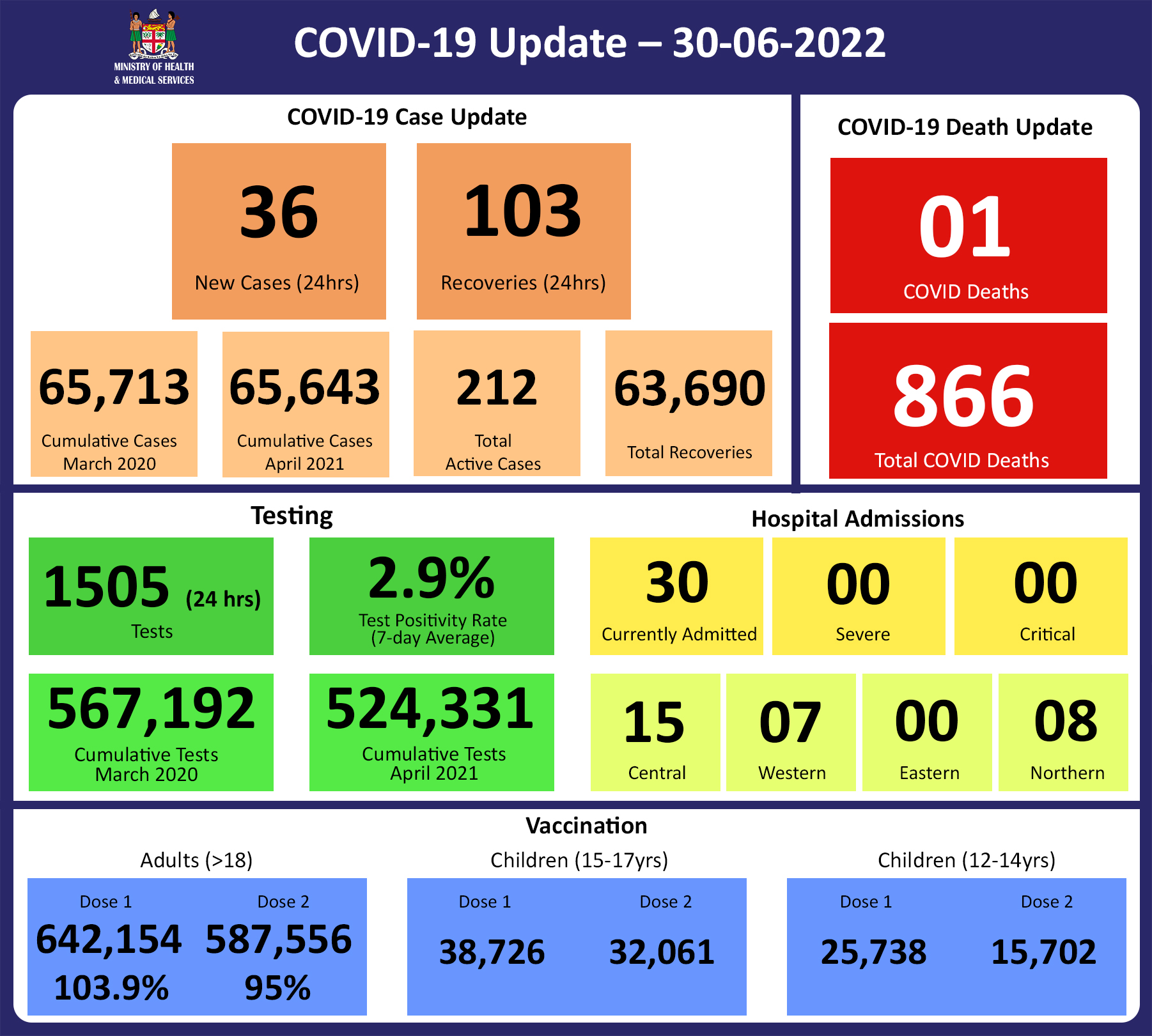
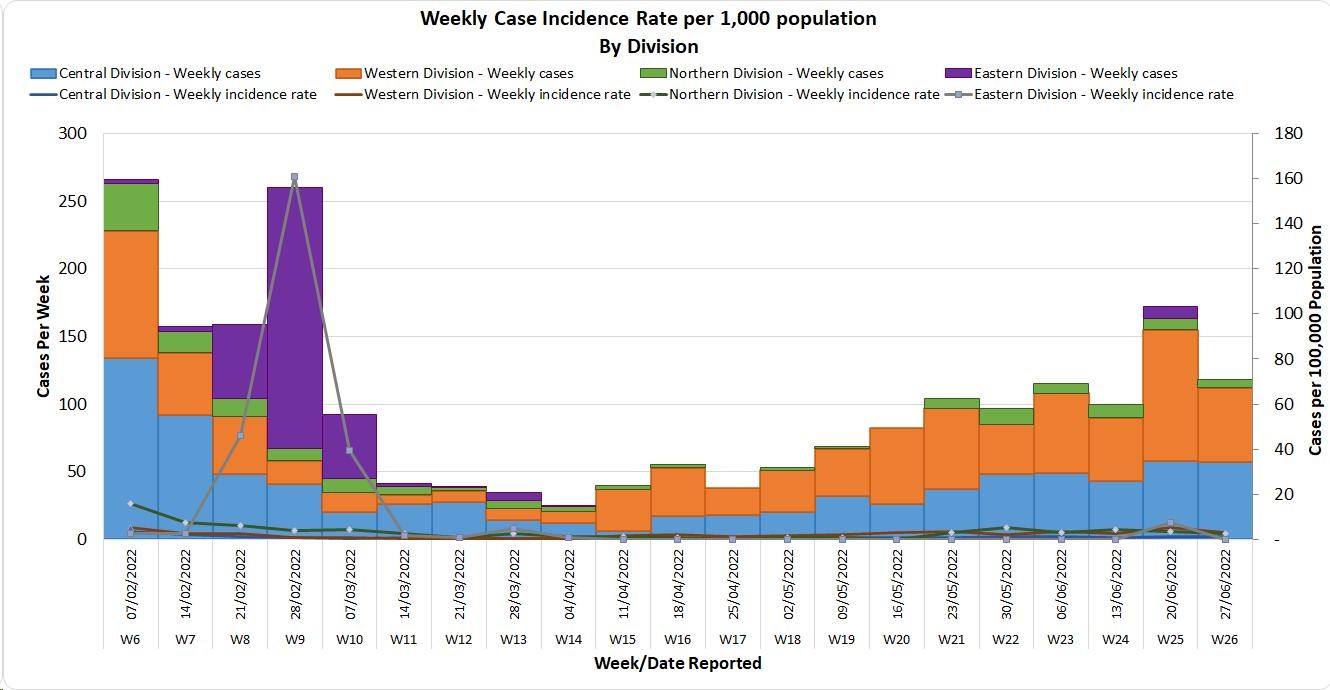
Since the last update, we have recorded 158 new cases of which 62 new cases were recorded on 28/06/2022; 60 new cases were recorded on 29/06/2022 and 36 new cases in the last 24 hours ending at 8 am this morning. Of the 158 cases recorded, 67 cases were recorded in the Central Division; 53 cases were recorded in the Western Division; 21 cases were recorded in the Northern Division and 17 cases were recorded in the Eastern Division. The national 7-day rolling average of cases as of 26th June is 30 daily cases. In the 7 days until 29/06/2022, 99 new cases were recorded in the Central division, 79 new cases in the Western division, 28 new cases in the Northern Division and 37 new cases in the Eastern Division. The Central Division cases constitute 67% of the cumulative total cases nationally, with the Western division making up 28%, 3% in the Northern Division, and 2% in the Eastern Division. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Deaths:
The curve depicts weekly COVID-19 deaths by division since May 2021. It indicates a surge from last December, with peaks in mid-January 2022 followed by a downward trend. The latest COVID death was reported on 11/06/22. COVID Death Reports We have one new COVID-19 death to report. The COVID-19 death is of an 89-year-old female from the Central Division who was brought to Valelevu Health Centre in distress on 28/06/2022. Sadly she passed away a few hours after the presentation. She had pre-existing comorbidities and was unvaccinated. Analysis of Deaths in the Third Wave Table 1: Death rates by Division
An analysis of the 165 deaths recorded in the third wave shows that, while the Western Division has the highest absolute number of deaths, the Northern Division has the highest rate of death when adjusted for population. Table 2: Deaths by Age Group
For the 165 deaths in the third wave, the death rate adjusted per 100,000 population, has been highest in age groups 50 and onwards. There were 8 deaths below the age of 19 years, 7 out of the 8 children had significant pre-existing medical conditions, and one child had no known underlying medical condition. Table 3: Deaths by Vaccination Status
Out of 165 COVID -19 deaths reported in the third wave, six (6) deaths were in the population not eligible for vaccination (under age 12). An analysis of the 159 deaths in the vaccine-eligible population reflected, that when adjusted per 100,000 population, for fully vaccinated (received 2 doses) and unvaccinated/not fully vaccinated (received 0 doses or only 1 dose) adults in Fiji, we have a death rate of 10.3 per 100,000 population for fully vaccinated adults and 313.5 per 100,000 population for unvaccinated adults. This means that unvaccinated adults in Fiji have been dying at a rate 30.4 times higher than fully vaccinated adults during the current COVID-19 wave. Individuals in the 12-17 age group who died were not vaccinated. There have been no COVID-19 deaths in individuals who received a booster (3rd dose) of the vaccine. There have been a total of 866 deaths due to COVID-19 in Fiji. As of June 26th, 2022, the national 7 days rolling average for COVID-19 deaths per day is now 0.0, with a case fatality rate of 1.29%. Due to the time required by clinical teams to investigate, classify and report deaths, a 4-day interval is given to calculate the 7 days rolling average of deaths, based on the date of death, to help ensure the data collected is complete before the average is reported. We have also recorded 943 COVID-19-positive patients who died from other serious medical conditions unrelated to COVID-19; their doctors determined that COVID-19 did not contribute to their deaths, therefore these are not classified as COVID-19 deaths. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hospitalization:
Using the WHO clinical severity classification, there are 93% (n=28) cases in the asymptomatic and mild categories; 7% (n=2) in the moderate category; and nil cases in the severe and critical categories. Anyone admitted to the hospital is tested before admission, therefore, a significant number of people are admitted to the hospital for non-covid health conditions, but incidentally, test positive due to the high amount of transmission in the community. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Testing:
1,505 tests have been reported for June 29th, 2022. Total cumulative tests since 2020 are 567,192 tests. The 7-day daily test average is 1,239 tests per day or 1.4 tests per 1,000 population. The national 7-day average daily test positivity is 2.9% which is within the WHO recommendation of 5%. |

Public Advisory
As we enter our cool and dry season we continue to record an increasing trend in respiratory infections, especially in children. An increase in admissions at the children’s hospital at CWMH was announced some weeks ago- samples collected from some hospitalised children tested negative for COVID-19 and influenza at Fiji CDC. A subset of samples sent to the Victorian Infectious Diseases Reference Laboratory in Melbourne detected seasonal respiratory viruses that cause the common cold but may cause severe respiratory illness in children under the age of 5. This is made up of a number of respiratory viruses that cause cold and flu symptoms. It has been expected that as restrictions intended to prevent transmission of COVID-19 were lifted (including mandatory masking, physical distancing, and school and border closures) other respiratory viruses that normally circulate would begin to re-emerge similar to pre-COVID levels, and possibly even at higher levels due to a decrease in population immunity to seasonal viruses, as cold/flu cases were low during the last two years.
For COVID 19;
- As reported, we continue to see an increasing trend. Recent severe diseases and deaths have been seen only in those with severe comorbidities (underlying illnesses). Also, they are either unvaccinated or have not received the booster dose that would be appropriate given the well-known recommendation for those with severe comorbidities to have at least one booster dose if not both. Unfortunately, we have another death to report in an 89-year-old female with co-morbidities who was unvaccinated. She presented very late for care.
- We also note an increase in cases admitted that are positive for COVID 19 and we are receiving reports of an increase in cases reported from workplaces. All the hospitals have been notified to reintroduce more stringent COVID safe measures. These include restricting visitors, more strict enforcement of masking and hand sanitization practices and to strengthen screening protocols. For workplaces, we strongly advise that COVID safe measures be more actively promoted and enforced by management.
- Private laboratories, GPs, and pharmacies that are part of the Ministry’s testing network (through application to the COVID Risk Mitigation Taskforce) are authorised to conduct COVID-19 testing and as such must comply with the established system of reporting positive and negative results to the MOHMS. Positive cases reported by private facilities to the MOHMS are reported in the regular public updates.
- Anyone who is sick should not be attending work or school. If you have COVID-19 symptoms you must get tested for COVID-19. If you test positive- isolation is mandatory for 7 days.
- Vaccines have provided a level of protection from severe disease and death such that the increasing trends in cases remain less of a concern. However, we have maintained a number of public health mandates and measures that relate to vaccination and incoming travel. The Ministry of Health and Medical Services envision that the more the booster dose the better the level of protection, and the safer it will be to remove the remaining public health measures further. The Ministry is currently looking at 80% booster coverage for those over 18 years of age.
We also note that we are in the middle of our chickenpox season, we have noted cases positive for measles and we have recorded cases of hand, foot and mouth disease; a disease that is caused by a family of viruses called enteroviruses. All these diseases can be mistaken for what many have read about monkeypox. We have yet to diagnose a case of monkeypox in Fiji. MOHMS have also released a number of advisories for the public. And we have released guidelines to all clinicians in public and private sectors in order to facilitate early case identification and reporting.
COVID-19 Vaccination
As of the 30th of June, a total of 141,572 individuals have so far received booster doses. This represents 45% of those eligible for a booster dose.
Increasing Vaccine Booster Coverage Program
It is well documented that immunity against COVID-19 infection acquired from COVID-19 vaccination wanes over time. The effectiveness of protection against COVID-19 after a primary series of AstraZeneca vaccination is slightly lower than with other COVID-19 vaccine products, especially against the Omicron variant of concern. However, receiving a third dose (booster), especially of an mRNA vaccine like Pfizer or Moderna, boosts immunity against infection.
There is also evidence that prior infection with a non-Omicron variant or the Omicron sublineages of BA.1 and BA.2 may not protect against infection with Omicron sublineages BA.4 and BA.5, which are now dominant in some countries- though some protection against severe disease is still expected. There is no evidence that BA.4 and BA.5 cause more severe disease than previous variants. The latest genomics sequencing results show that Omicron sublineages BA.1 and BA.2 are in circulation in Fiji, while BA.4 and BA.5 have not yet been detected.
This means that, once these sub-lineages enter the community, it is expected that people may get infected, even if they have been infected before; and while the risk of severe disease is expected to remain low in those who have had 2 doses and have no underlying illnesses, increased sickness may still have a negative impact on the workforce. And people with underlying conditions like diabetes, heart disease, kidney disease etc. will h. will continue to be at higher risk of severe disease and death.
These considerations, and the current noticeable increase in cases, indicate an urgency to increase our efforts to increase booster dose coverage. The return of most of the medical immunisation staff has also helped to ensure support for escalating our vaccine booster coverage program.
Based on this and international evidence the Ministry recommends the booster dose interval for eligible persons over 18 years be reduced to 3 months after the 2nd dose in recognition;
- of the risk of disease surge based on waning 2 doses of COVID-19 vaccine protection
- slow booster uptake
- increased international travel with the relaxation of border measures
- ongoing outbreaks in various parts of the world with an increase in Omicron sublineages that may evade infection-induced immunity from other variants
Hence, we urge the public to get booster vaccine doses with a list of vaccination sites provided daily by the MHMS. Currently, both Pfizer and Moderna are recommended for booster doses.
In order to optimise coverage, the aim of the booster campaign is to administer 250,000 doses of Pfizer vaccine to those who have completed the primary series (doses 1 and 2) > 3 months prior but have not yet received a booster dose. This requires a minimum of 32,000 doses to be administered weekly for 8 weeks from 1 June to 31 July 2022.
COVID-19 booster priority populations are;
- Persons over the age of 18 years who have completed their primary series > 3 months prior can receive their 1st booster dose
- Immunocompromised persons and those over the age of 60 years who had received the 3rd booster dose, may receive the 4th dose after a period of 4 months
- Health care workers, port staff, tourism and others who wish to receive a 2nd booster dose may receive it after an interval of 4 months from their first booster dose.
- Anyone over 18 years who have taken their 1st booster dose can receive a 2nd booster dose after an interval of 4 months.
- Micro planning workshops commenced in the Central Division on 30th May 2022. Western and Northern Division will start on 6th June 2022. Follow-up supervisory visits will occur weekly until the end of June.
International communicable disease outbreaks
As previously mentioned, the Ministry’s Fiji Centre for Disease Control (Fiji CDC) and Border Health Protection Unit (BHPU) are monitoring international outbreaks of concern, which include Ebola Virus Disease in the Democratic Republic of Congo, Japanese Encephalitis in Australia, acute hepatitis of unknown origin in multiple countries, and monkeypox in the United Kingdom and other countries. Where appropriate, specific interventions have been put in place or strengthened in response. The situation will continue to be monitored, assessed, and responded to based on the available scientific evidence, best practice, and advice from expert authorities.
Monkeypox
We can confirm that the 3 cases under investigation for monkeypox have tested negative. Our current position is that while monkeypox spreads worldwide, the evidence remains that monkeypox does not spread easily between people unless there is close contact. It is also amenable to localised public health measures with minimal to low social and economic impact. At present WHO does not recommend that the Member States adopt any measures that interfere with international traffic for either incoming or outgoing travellers.
Person-to-person transmission may occur through;
- contact with clothing or linens (such as bedding or towels) used by an infected person
- direct contact with monkeypox skin lesions or scabs
- exposure to respiratory droplets eg coughing or sneezing
The Ministry of Health and Medical Services continues screening persons of interest and investigating cases that demonstrate symptoms similar to what is seen in monkeypox.
Monkeypox is usually a self-limiting illness, which means that most people recover with just supportive (symptom relief) treatment within several weeks. However, severe illness can occur in some individuals. We are also in discussions with development partners to see if we can preposition access to vaccines and medications used to treat monkeypox.
As previously mentioned, our response plan includes surveillance with rapid response and containment protocols. A key focus will be on ensuring that those suspected or confirmed to have monkeypox must be managed dignifiedly with no threat of stigmatisation. Each citizen’s duty to contribute to protecting Fiji must be the priority.
The Ministry has been working with communications and community engagement teams to produce public advisories to help arm ourselves with the knowledge to protect ourselves and to help reduce the chances of spread in our community. Infection prevention protocols have been put together at the border and in community facilities. Protocols have been initiated to maintain oversight over travellers from selected countries to ensure early diagnosis, treatment, and contact tracing. The public advisories have covered symptoms to enable the public to quickly recognize symptoms and seek medical care while preventing transmission to others.
All doctors and Nurses in the community need to ensure they are well informed of how cases present and be vigilant in helping to ensure cases are diagnosed early. The Ministry’s guidelines for early detection and response, as well as laboratory testing, have been distributed to all public and private clinicians.
Discussions with our reference laboratory in Melbourne are in place to ensure access to definitive tests. Our ongoing efforts to have genomic sequencing capability in the Fiji CDC will provide us with greater capacity to deal with infection threats now and in the future.
As we escalate our community-wide infection prevention and control measures, we are responding to current threats and creating community-wide resilience to upcoming threats. Our ongoing engagement in a healthy lifestyle to mitigate NCDs is also part of the overall focus on building back better and stronger.
The Ministry of Health and Medical Services will continue to disseminate more specific advisories over the coming weeks. Further updated knowledge about the monkeypox virus will be shared as they are known.
Ongoing Medical Recovery Efforts
With reducing COVID-19 cases and people presenting to health centres with acute respiratory illness, the MOHMS team is better positioned to focus more on health facilities and health care provision capabilities to mitigate against severe disease and death. This will include the ongoing community engagement and outreach program to facilitate early diagnosis and treatment in the community, and the maintenance of health facility readiness to provide treatment.
We have received a large number of drugs and consumables that have finally arrived and a nationwide deployment effort is currently underway to facilitate the delivery of these items to all our medical facilities. Also, a supply chain management digital platform has been launched and we expect to see improvements in the supply of consumables and medicines as a result of these initiatives.
Our command and operation centres have been repurposed to maintain a line list of vulnerable cases in the community and work on processes that will allow for more preemptive response and promote broader community resilience. These command centres and operation centres will also provide oversight on community surveillance indicators to ensure early and measured responses to future outbreaks.
We are also focused on carrying out general health service work more efficiently in all facilities, and a key part of our plan is to set up divisional mobile units to supplement facility-based general servicing capability and also work with private providers through a process for pre-qualifying contractors and/or suppliers for each subdivision.
The engagement of General Practitioners, Private Dental Practitioners, Private Medical Laboratories, and Private Ambulance providers to support our services in a public-private partnership arrangement is a strategy to help in our ongoing recovery efforts.
We also have reformulated a framework to better engage customer service initiatives in all health facilities and allow for senior managers to institute substantive actions and provide direct oversight over implementation plans. It will also allow the Ministry’s senior executives to track progress in implementation and ensure that annual operation plans reflect an evolving and progressive change narrative in the successive plans. These initiatives will also include the processing of internal communications to facilitate timely decision-making and action within the Ministry.